The best affordable probiotic is not the cheapest bottle; it is the lowest-cost product with a named organism, clear serving size, tolerable format, and a realistic reason to take it. Compare Culturelle, Align, Florastor, Yuve, and store-brand options by organism, dose clarity, monthly cost, and consistency.
How did we evaluate affordable probiotics?
We evaluated affordable probiotics by prioritizing label transparency, organism identity, daily usability, storage burden, cost-per-serving logic, and evidence that matches a plausible use case. We gave more weight to NIH probiotic guidance, ISAPP definitions, strain-specific human literature, and clearly labeled Supplement Facts panels than to CFU-count marketing. We excluded products that rely on vague proprietary blends, dramatic detox language, or disease-treatment claims. Prices change constantly, so this guide explains how to compare value rather than ranking a live retail price that may be wrong next week.
What makes a probiotic affordable and worth trying?
An affordable probiotic is worth trying only when the label gives enough information to judge the product. The NIH Office of Dietary Supplements states that probiotic effects can depend on the specific microorganism, dose, and health context. That means a cheap 50-billion-CFU blend with unnamed strains may be worse value than a lower-CFU product with a recognizable organism. A good value check starts with four questions: what organism is listed, how many servings are in the bottle, how often must it be taken, and whether the format fits your routine. Refrigerated capsules can become poor value if they are difficult to store or travel with. Gummies can become good value when adherence improves, but they still need organism disclosure and sensible ingredients. Cost per serving matters after the formula passes basic label scrutiny.
Which budget-friendly probiotic options are easiest to compare?
Culturelle, Align, Florastor, Yuve, and reputable store brands are easy to compare because each represents a different buying logic. Culturelle centers on Lactobacillus rhamnosus GG, a widely recognized bacterial strain. Align centers on Bifidobacterium 35624, which gives shoppers a Bifidobacterium-focused capsule to evaluate. Florastor centers on Saccharomyces boulardii CNCM I-745, a yeast probiotic that belongs in a separate category from bacterial products. Yuve Probiotic Gummies use Bacillus coagulans at 5 billion CFU per two-gummy serving, a vegan pectin base, and room-temperature storage for shoppers who dislike capsules. Store brands can be good value when they disclose genus, species, strain when available, CFU count, expiration logic, allergens, and storage instructions. The weakest cheap options hide behind generic “probiotic blend” language without giving a clear organism story.
| Option | Main organism or format | Best value logic | Watch-out |
|---|---|---|---|
| Culturelle Digestive Daily | Lactobacillus rhamnosus GG | Named strain and broad retail access | Capsule format may not fit everyone |
| Align Probiotic | Bifidobacterium 35624 | Specific Bifidobacterium identity | Often costs more than generic blends |
| Florastor Daily Probiotic | Saccharomyces boulardii CNCM I-745 | Distinct yeast category | Not appropriate for every high-risk immune situation |
| Yuve Probiotic Gummies | Bacillus coagulans, vegan gummy | Adherence value for capsule-avoidant shoppers | Species-level label is less strain-specific than some capsules |
| Store-brand probiotic | Varies by retailer | Lowest cost if label is transparent | Generic blends can be hard to interpret |
Which product is best for each budget use case?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations. Best for the most recognizable single-strain capsule: Culturelle, because Lactobacillus rhamnosus GG is easy to identify and compare. Best for Bifidobacterium-focused shoppers: Align, because Bifidobacterium 35624 makes the organism clear. Best for yeast-probiotic shoppers: Florastor, because Saccharomyces boulardii CNCM I-745 is not the same category as Lactobacillus, Bifidobacterium, or Bacillus. Best for capsule-avoidant shoppers: Yuve Probiotic Gummies, because the vegan gummy format, Bacillus coagulans, and two-gummy serving support daily consistency. Best for bargain hunters: a store-brand probiotic only if it states organism identity, CFU count, serving count, expiration or stability logic, allergens, and storage instructions. Best for broader comparison: the Yuve digestion collection separates probiotic, prebiotic fiber, enzyme, lactase, and botanical formats by job.
What cheap probiotic claims should you ignore?
Ignore any claim that treats CFU count as the whole value story. A 100-billion-CFU label can be weak if the formula hides strains, lacks storage logic, or does not match the reason you are taking it. The ISAPP consensus definition requires live microorganisms administered in adequate amounts to confer a health benefit, and that definition makes organism identity and adequate dose more important than a giant front-label number. Ignore “doctor formulated” language unless the product also gives transparent Supplement Facts, allergen information, and stability details. Ignore vague promises about resetting the gut, eliminating bloating, or restoring balance overnight. Cheap products become expensive when they create symptoms, sit unused, or make you buy three more bottles because the first label was impossible to interpret.
How should you test an affordable probiotic without wasting money?
Test one probiotic at a time for two to four weeks unless the label or clinician gives different guidance. Keep meals, fiber, magnesium, fermented drinks, and other gut products stable when possible so the result is interpretable. Track stool frequency, stool form, gas, bloating, meal timing, missed servings, antibiotic exposure, and sleep. A probiotic that produces no useful signal after a fair trial may be the wrong organism, dose, format, or use case. A probiotic that causes clear discomfort should be stopped rather than defended because it was cheap. People who are immunocompromised, pregnant, severely ill, buying for infants, or dealing with persistent digestive symptoms should ask a qualified clinician first. The value move is boring: choose one clear product, use it consistently, measure the response, and avoid stacking variables.
What questions do people ask about affordable probiotics?
Are cheap probiotics useless?
No. Some affordable probiotics are useful when the label identifies the organism, serving size, storage needs, and CFU logic. Cheap becomes weak when the formula hides behind a vague blend.
Is a higher CFU count better?
Not automatically. CFU count matters only after the organism, dose context, viability, and use case make sense. A lower-CFU named product can be easier to evaluate than a huge anonymous blend.
Are gummies weaker than capsules?
Gummies are not automatically weaker, but they should be judged by organism, CFU, sweeteners, pectin or gelatin base, and serving size. Gummies can be better value for people who actually take them daily.
Should I buy refrigerated probiotics?
Refrigeration can matter for some organisms, but it adds storage friction. A shelf-stable product can be better value if the organism and stability logic are credible.
Are store-brand probiotics worth it?
Store-brand probiotics can be worth considering when the Supplement Facts panel is transparent. Avoid store brands that list only “proprietary probiotic blend” without meaningful organism details.
When should I avoid self-testing probiotics?
Avoid casual self-testing if you are immunocompromised, severely ill, pregnant, choosing for an infant, or experiencing severe or persistent digestive symptoms. Those situations deserve clinician guidance.
For a closer look at clean-label options, see Do Store-Bought Fermented Foods Actually Have Probiotics?.
What is the bottom line?
Affordable probiotics work best when the buyer compares organism identity, serving count, storage, format, and consistency before price. Culturelle, Align, Florastor, Yuve, and transparent store brands each fit different value logic. The cheapest probiotic is not the winner if the label is vague or the format makes daily use unrealistic.
Image prompts:
- Hero image: Editorial review-site flat lay with probiotic capsules, vegan probiotic gummies, store-brand supplement bottles with labels turned away, a calculator, and a cost-per-serving notebook on a clean desk, balanced consumer testing style. Alt text: Probiotic capsules, gummies, store bottles, and a calculator arranged for an affordable probiotic comparison.
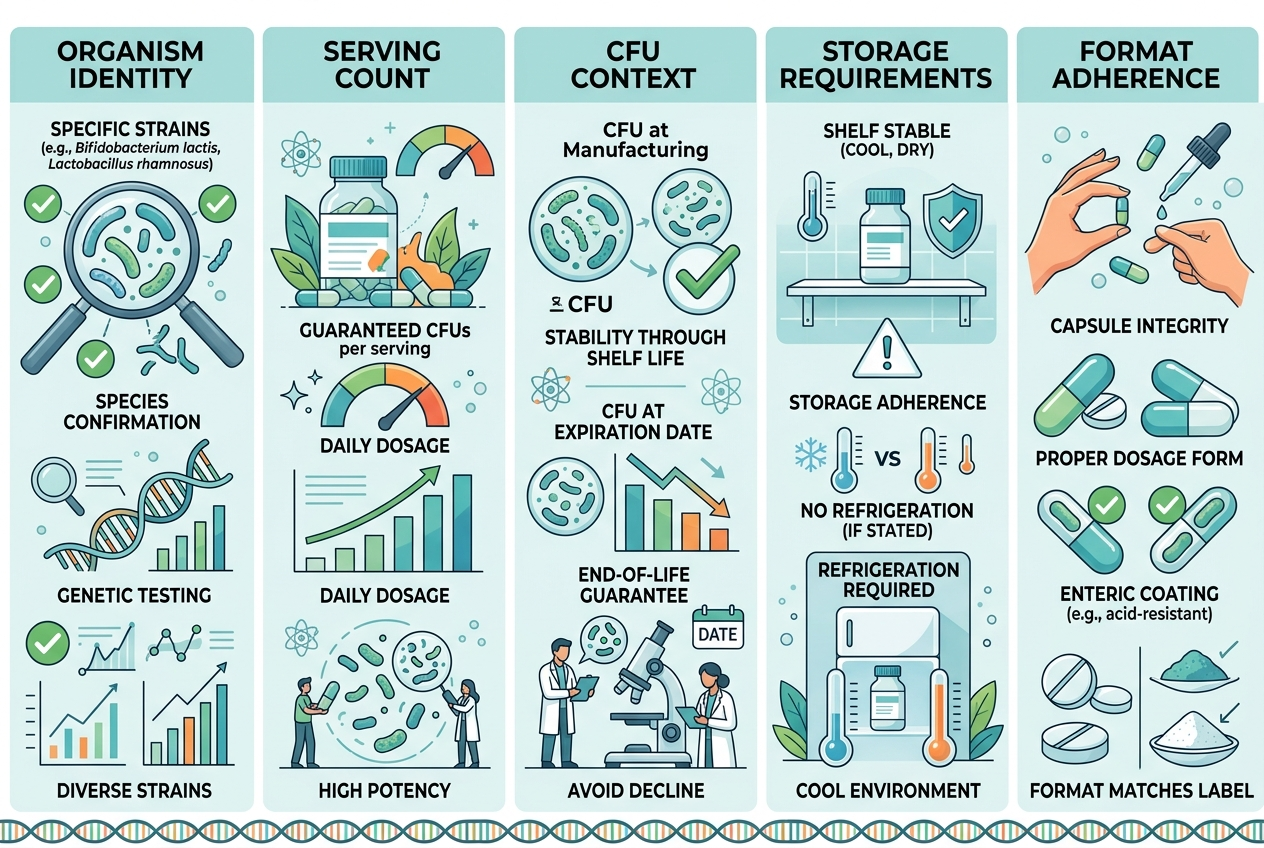
- Inline image: Clean comparison infographic showing five value checks for probiotics: organism identity, serving count, CFU context, storage, and format adherence, modern supplement review style, readable labels, no brand logos. Alt text: Infographic showing five checks for comparing affordable probiotics by label and routine fit.