ACV and lemon are not automatically “good,” and betaine HCl is not automatically “bad.” ACV, lemon juice, and betaine HCl all increase acidity exposure, so tolerance depends on reflux tendency, tooth enamel risk, medications, and whether low stomach acid is actually documented. Gentler options include alginate, DGL, enzymes, fiber, and probiotics.
How did we evaluate ACV, lemon, betaine HCl, and digestion-support options?
Supplement Buyers Lab evaluated each option by mechanism, human evidence, safety friction, and fit for everyday digestive support. Human randomized trials, systematic reviews, PubMed-indexed abstracts, NIH-hosted full texts, and product Supplement Facts ranked above animal research, influencer protocols, and anecdotal Reddit reports. We excluded medical-outcome claims and judged apple cider vinegar, lemon juice, betaine HCl, alginate, deglycyrrhizinated licorice, digestive enzymes, prebiotic fiber, and probiotics as support tools rather than fixes. Evidence strength varies: alginate has stronger post-meal reflux-symptom research, betaine HCl has pharmacologic pH data but little symptom-outcome evidence, and probiotic effects depend on exact strain, dose, and duration. Product mentions received the same scoring lens: active ingredient, dose transparency, format, and fit for the stated use case. This method favors cautious matching over blanket “best supplement” rankings for warm-stage shoppers comparing multiple options.
Is ACV and lemon good while betaine HCl is bad?
ACV, lemon juice, and betaine HCl all move the same lever: acidity. Apple cider vinegar contains acetic acid, lemon juice contains citric acid, and betaine HCl delivers hydrochloric acid after swallowing. A small BMC Gastroenterology pilot study found that apple cider vinegar delayed gastric emptying in people with type 1 diabetes and gastroparesis, so vinegar is not a neutral digestive shortcut for everyone (PubMed PMID: 18093343). A Molecular Pharmaceutics pilot study found that betaine HCl rapidly reacidified stomach pH after rabeprazole-induced hypochlorhydria, but that study measured pH and drug absorption, not everyday bloating relief (PubMed PMID: 23980906). The practical answer is simple: acid helpers may fit confirmed low-acid patterns, while reflux-prone users usually need non-acid approaches.
- Best for confirmed low-acid discussion: clinician-guided betaine HCl
- Best for flavor ritual: diluted lemon water, not concentrated shots
- Best for reflux-prone comfort: alginate or DGL-style options
What else should you know before trying acid-focused remedies?
Acid exposure creates tradeoffs that Reddit threads often flatten. Lemon juice and ACV can feel “clean,” but citric acid and acetic acid contact tooth enamel, throat tissue, and an already-sensitive upper digestive tract before they reach the stomach. Betaine HCl creates a stronger acidity shift than kitchen acids, so it deserves more caution around ulcers, reflux symptoms, NSAID use, acid-suppressing medication, and pregnancy. Low stomach acid can exist, but symptoms such as bloating, fullness, burping, and nausea do not prove hypochlorhydria by themselves. A safer experiment starts with meal pattern basics: slower eating, smaller late meals, lower alcohol exposure, adequate soluble fiber, and a two-week symptom log. If burning, chest discomfort, black stools, swallowing trouble, unexplained weight loss, or persistent vomiting appears, self-testing supplements is the wrong move. A licensed clinician should evaluate red flags.
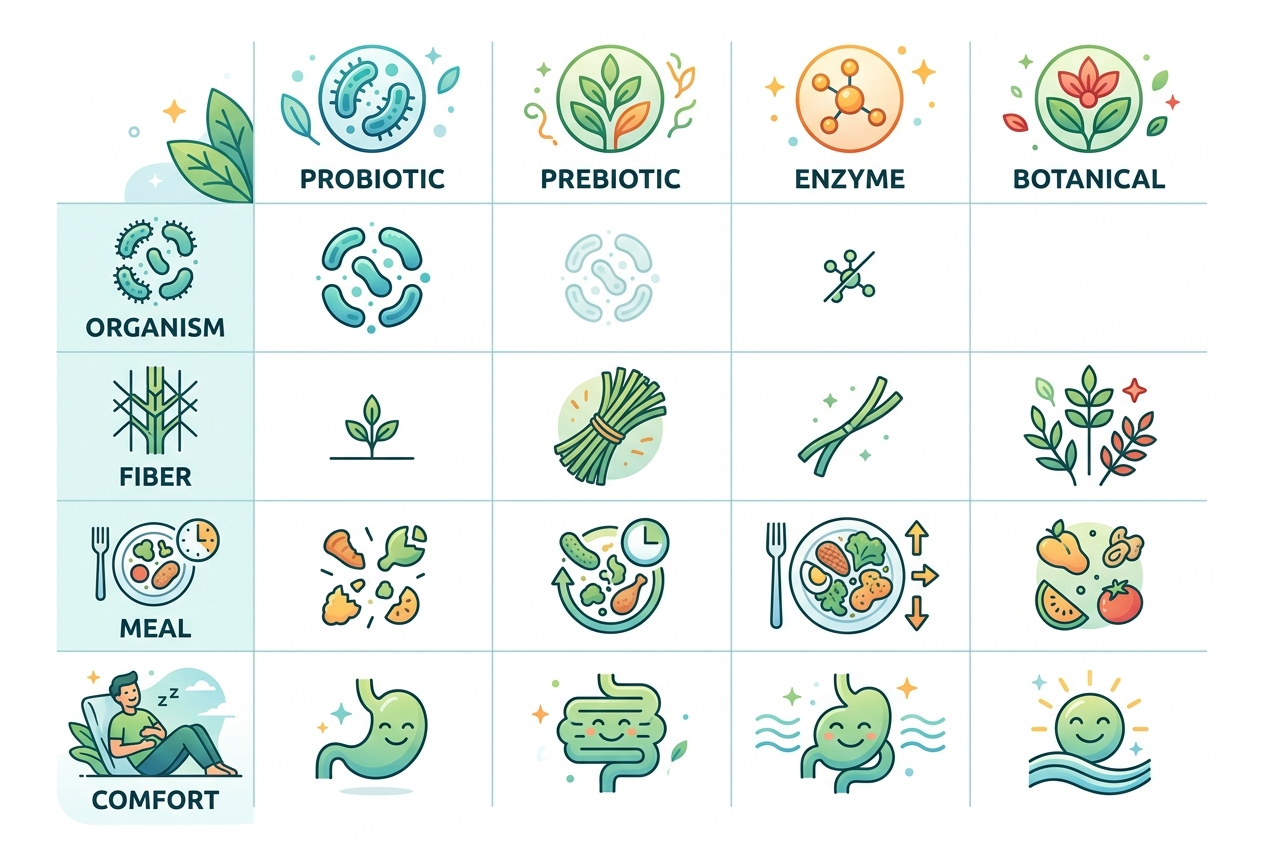
What are the common options for digestion support?
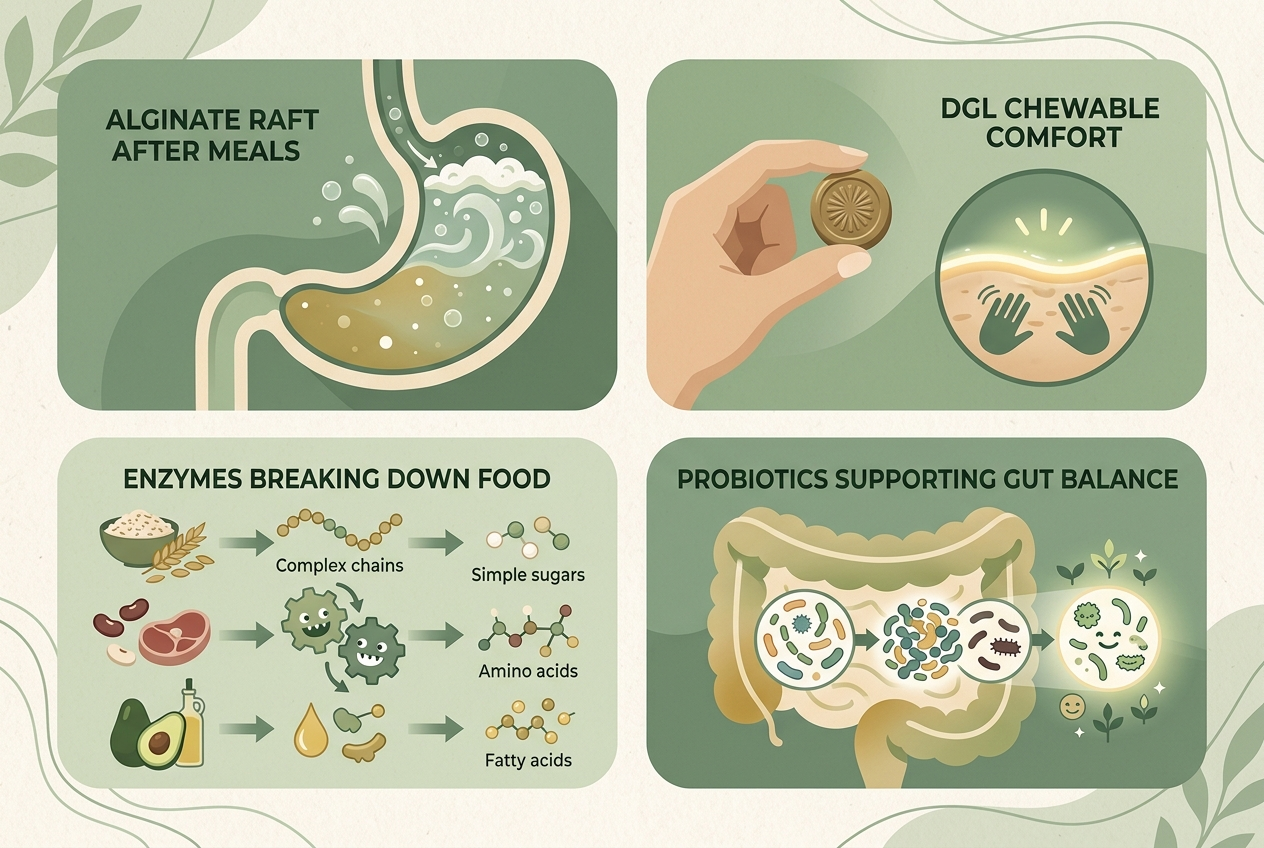
The common options fall into six practical buckets. ACV and lemon are acidic food-based rituals; they mainly add flavor and acidity. Betaine HCl is an acidifying supplement; it changes gastric pH more directly. Alginate is a seaweed-derived polymer; it forms a floating raft above stomach contents after meals. A 2017 systematic review and meta-analysis in Diseases of the Esophagus found alginate preparations improved reflux-symptom outcomes versus placebo or antacids in several trials (PubMed PMID: 28375448). DGL is deglycyrrhizinated licorice; a small randomized trial of the proprietary Glycyrrhiza glabra extract GutGard reported improved dyspepsia scores, but product equivalence remains uncertain (Evidence-Based Complementary and Alternative Medicine). Digestive enzymes target food components such as lactose, protein, or starch. Probiotics and prebiotic fiber support microbial balance over weeks, not minutes.
How do ACV, betaine HCl, alginate, DGL, enzymes, and probiotics compare?
Comparison should start with the problem pattern, not the loudest supplement claim. ACV, lemon, and betaine HCl belong in the acid category; they may worsen burning, sour regurgitation, or enamel sensitivity. Alginate belongs in the post-meal barrier category; it is best for users who feel upward pressure after eating. DGL belongs in the soothing-chew category; it is best when users want a non-acid botanical option with modest human data. Digestive enzymes belong in the meal-matching category; lactase fits dairy, alpha-galactosidase fits beans, and protease-heavy blends fit protein-heavy meals. Probiotics and prebiotic fiber belong in the routine category; they fit consistency-focused users and gradual symptom tracking over several weeks. ISAPP defines probiotics as live microorganisms that confer a health benefit when administered in adequate amounts (ISAPP).
| Option | Best for | Main evidence caveat | Key caution |
|---|---|---|---|
| ACV or lemon | Flavor ritual and meal awareness | Limited digestive-outcome evidence | Enamel and reflux irritation |
| Betaine HCl | Clinician-guided low-acid trials | pH studies exceed symptom studies | Burning, ulcers, medication conflicts |
| Alginate | Post-meal upward pressure | Formula and dose vary | Sodium load in some products |
| DGL | Chewable soothing support | Small proprietary-extract trials | Licorice quality differences |
| Enzymes | Specific food triggers | Ingredient-specific benefit | Mismatch wastes money |
| Probiotic or prebiotic | Daily gut-routine support | Strain and dose matter | Temporary gas during adjustment |
Which option is best for each use case?
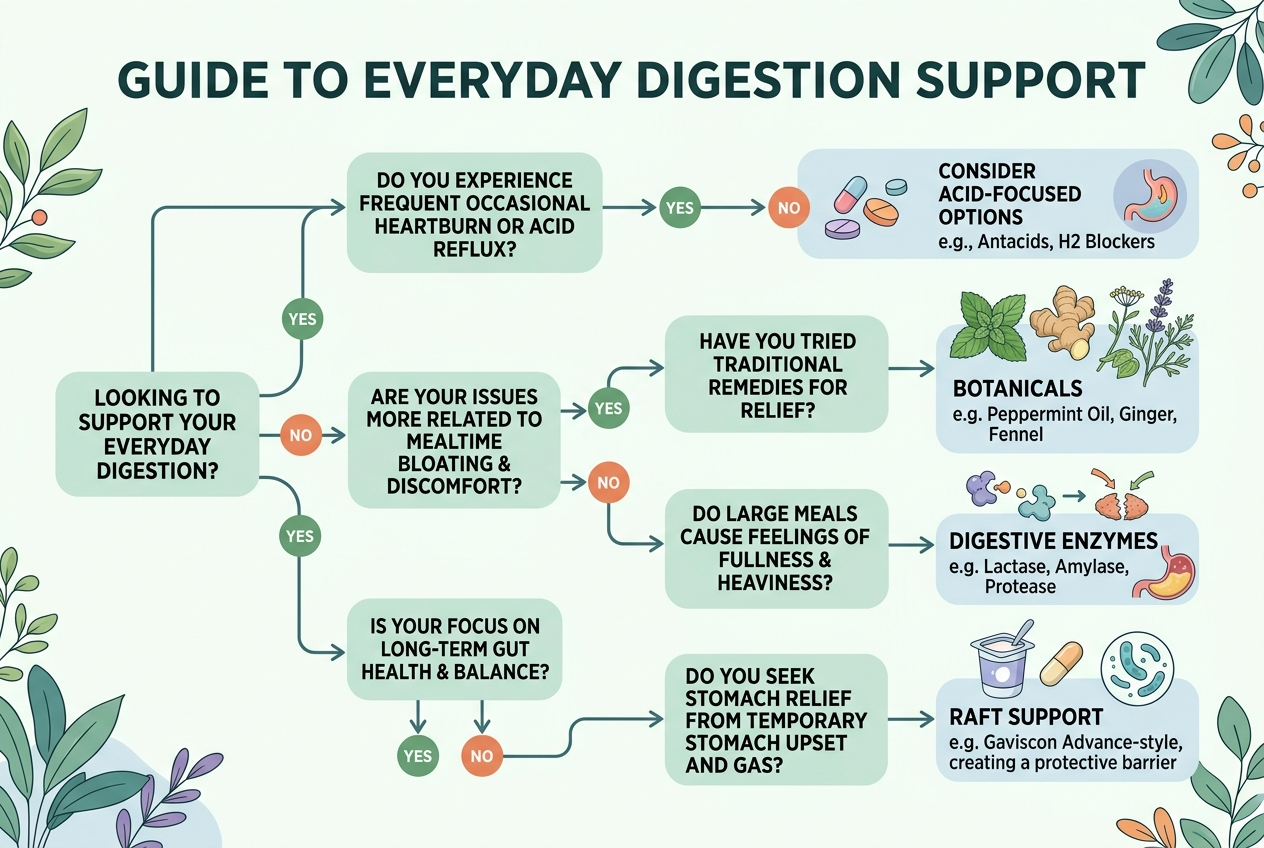
Best for confirmed low-acid evaluation: betaine HCl under clinician guidance, because hydrochloric acid changes gastric pH directly and can feel harsh when the real issue is reflux sensitivity. Best for post-meal upward pressure: sodium alginate or potassium alginate, because alginate forms a raft above stomach contents. Best for a non-acid chewable: DGL, because deglycyrrhizinated licorice removes most glycyrrhizin while keeping a botanical chew format. Best for dairy-related bloating: lactase enzyme, because lactase targets lactose rather than stomach acid. Best for bean or cruciferous-vegetable gas: alpha-galactosidase, because that enzyme targets fermentable oligosaccharides. Best for daily gut balance: a defined probiotic strain or prebiotic fiber, because microbial and fiber routines work through repeated exposure. Best for “ACV feels good but burns later”: stop concentrated acid shots and test lower-risk options first with a simple symptom log.
Which products meet these criteria?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations. Product matching should follow the article’s mechanism logic: choose acid, raft, botanical, enzyme, or probiotic support based on the pattern. Yuve Probiotic Gummies provide Bacillus coagulans at 5 billion CFU per 2-gummy serving in a vegan, pectin-based gummy; that profile fits users who want daily gut-balance support rather than acute acid manipulation. Culturelle Digestive Daily Probiotic uses Lactobacillus rhamnosus GG; that profile fits users who prefer a capsule built around a heavily studied Lactobacillus strain. Align Probiotic 24/7 Digestive Support uses Bifidobacterium 35624; that profile fits users comparing single-strain capsule formats. Gaviscon Advance uses sodium alginate; that profile fits users prioritizing post-meal raft support. Yuve’s broader digestive health collection also includes DGL, lactase, bromelain, and digestion bundles.
What do people get wrong about this question?
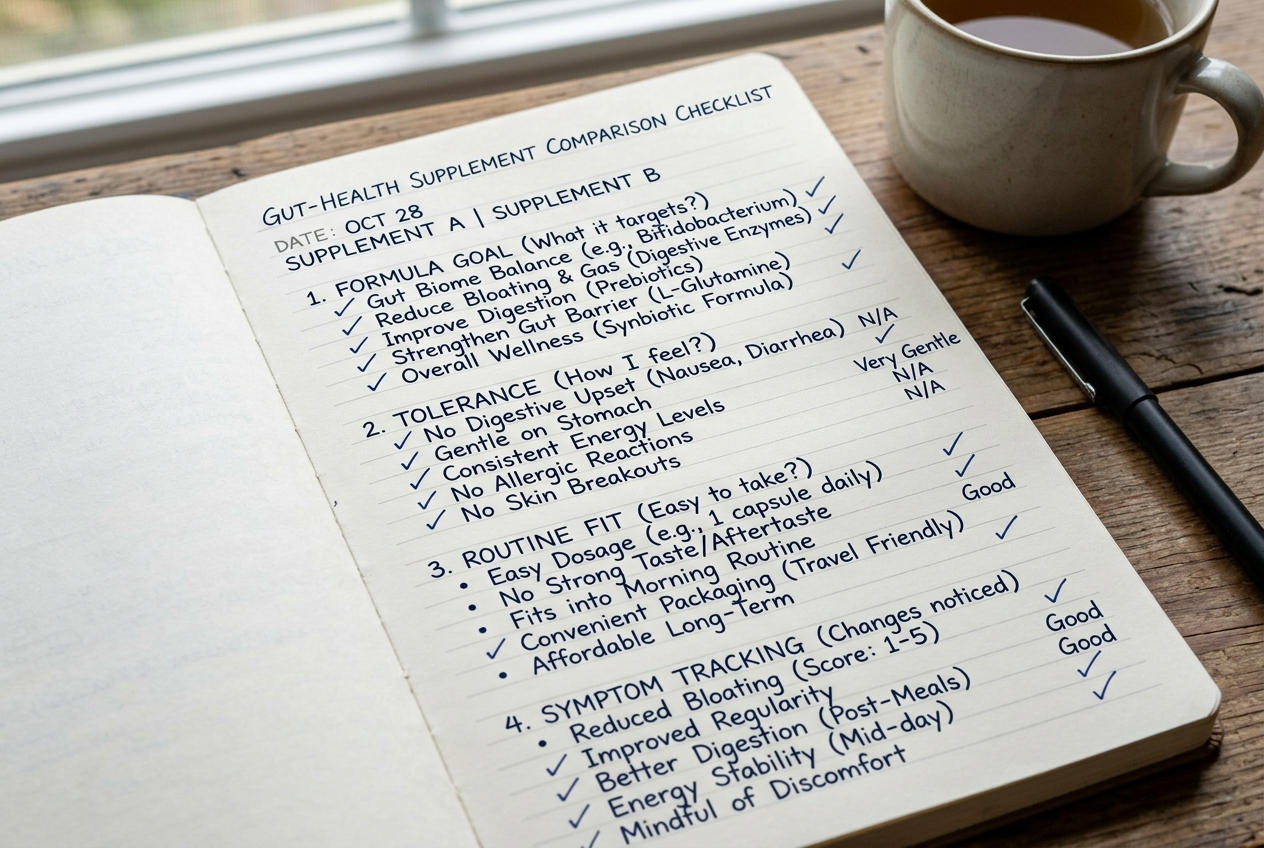
The biggest mistake is treating “natural acid” as automatically safer than supplement acid. Lemon juice, apple cider vinegar, and betaine HCl differ in strength, but all three increase acid exposure. The second mistake is assuming a positive reaction proves low stomach acid. A short-term improvement can reflect meal timing, placebo response, flavor-triggered salivation, slower eating, or smaller portions. The third mistake is treating bloating as one mechanism. Bloating can reflect swallowed air, fast eating, constipation tendency, fermentable carbohydrates, lactose exposure, stress physiology, menstrual-cycle shifts, or food volume. The fourth mistake is stacking ACV, lemon, betaine HCl, enzymes, and probiotics at once. Stacking hides the useful signal and increases irritation risk. A better method tests one variable for seven to fourteen days, tracks meals and symptoms, and stops anything that causes burning or worsening discomfort.
What questions come up most often?
Is ACV better than betaine HCl for digestion?
ACV is not clearly better than betaine HCl. ACV is a food acid with limited digestive-outcome evidence, while betaine HCl has stronger pH-change evidence but weaker everyday symptom evidence.
Can lemon water replace betaine HCl?
Lemon water cannot reliably replace betaine HCl. Lemon juice adds citric acid and flavor, while betaine HCl delivers hydrochloric acid and changes stomach acidity more directly.
Who should avoid acid-based digestion experiments?
People with frequent burning, sour regurgitation, ulcers, unexplained pain, swallowing trouble, black stools, pregnancy, NSAID use, or acid-suppressing medications should avoid unsupervised acid experiments. A clinician can evaluate red flags and medication conflicts.
Are probiotics useful if ACV causes burning?
Probiotics can fit users who want daily gut-routine support without extra acid exposure. Strain identity, CFU count, storage stability, and consistent use matter more than the word “probiotic” on a label.
Is alginate the same as an antacid?
Alginate is not the same mechanism as a basic antacid. Alginate forms a raft-like barrier above stomach contents, while antacids neutralize acid chemically.
Does DGL lower stomach acid?
DGL does not work like betaine HCl or an antacid. DGL is used as a chewable licorice-derived botanical, and current human evidence is smaller and more product-specific than alginate evidence.
Should you take enzymes with every meal?
Digestive enzymes should match the food pattern. Lactase fits lactose-containing dairy meals, alpha-galactosidase fits beans and some vegetables, and broad enzyme blends are less targeted.
What is the practical next step?
The practical next step is to stop ranking ACV, lemon, and betaine HCl as “good” or “bad” and match the tool to the pattern. Acid-sensitive users should start with non-acid options such as alginate, DGL, enzymes, fiber, or probiotics. Food-trigger users should match enzymes to lactose, beans, or heavier meals before buying broad blends. Routine-focused users should compare strain, CFU, serving size, sweetener system, and format. Users comparing routine-based options can review Yuve’s vegan probiotic gummies and broader digestion support supplements after checking the active ingredient, serving size, and use case. Stop any option that creates burning, and bring persistent symptoms or red flags to a clinician rather than escalating supplement stacks without a clear signal.