
Low fiber intake can contribute to loose, erratic bowel patterns in some people, but it does not by itself create an IBS-D diagnosis. Fiber type matters more than simply eating more fiber. Soluble fibers such as psyllium can add form, while fast-fermenting fibers can increase urgency or gas in sensitive people.
How did we evaluate low-fiber-related diarrhea patterns?
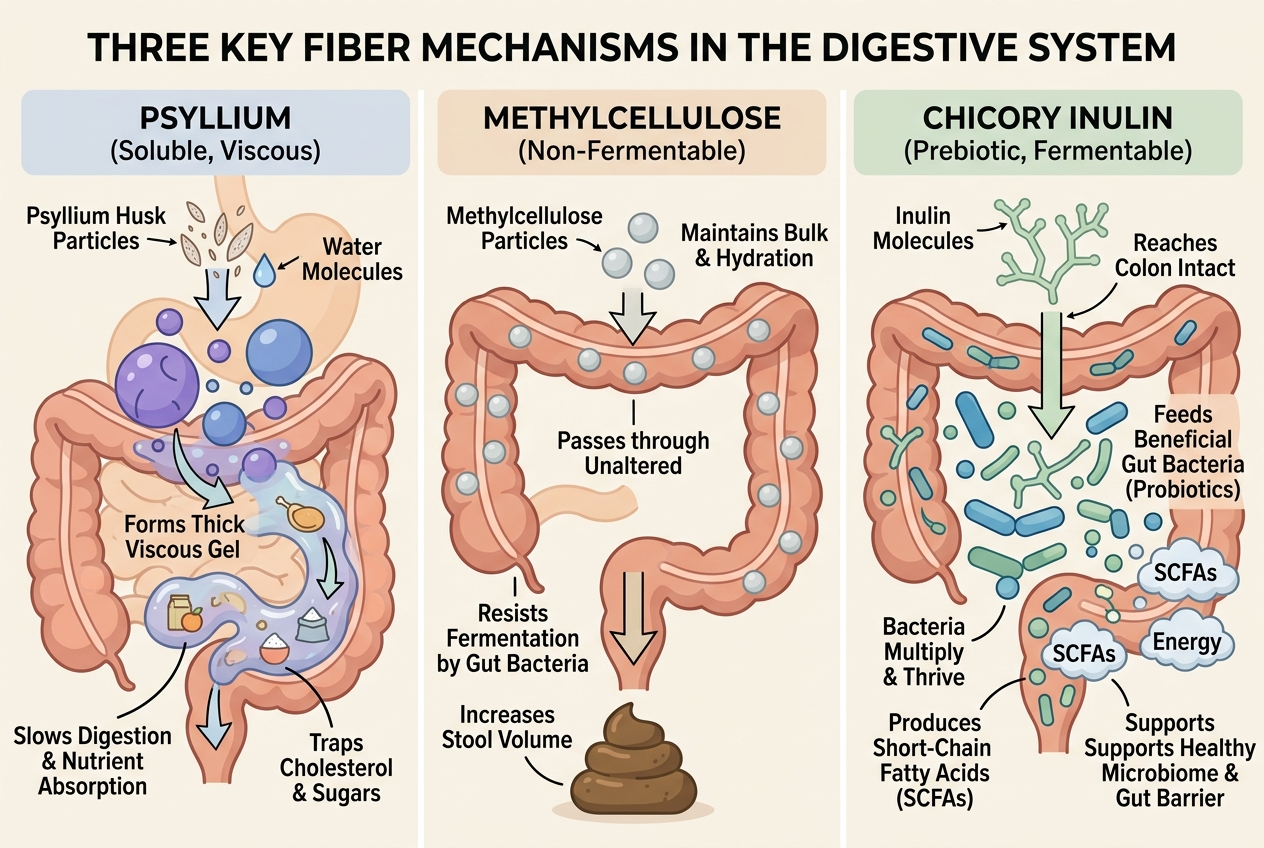
We evaluated this topic with a simple rule: human evidence outranked supplement marketing. We prioritized the American College of Gastroenterology guideline, randomized controlled trials, and meta-analyses on soluble fiber, stool form, and fermentable prebiotics, including the Moayyedi meta-analysis and the Nagy systematic review. We compared options by fiber type, dose per serving, fermentability, delivery format, and how well each option fits someone whose bowel pattern already feels unpredictable. We excluded disease-treatment claims, dramatic before-and-after promises, and vague “gut reset” language because those claims do not help a warm-stage buyer choose responsibly. We also treated label facts and ingredient mechanisms separately: psyllium can thicken stool, methylcellulose can add bulk with less fermentation, and chicory inulin can feed bifidobacteria but may feel too active for some people.
Can low fiber intake actually trigger diarrhea-like patterns?
Low fiber intake can reduce stool bulk, which means intestinal fluid has less material to bind to and stools can look looser or less formed. That pattern still differs from an IBS-D diagnosis, because IBS-D requires a broader symptom pattern and clinical context, not just one low-fiber week. Evidence supports soluble fiber more strongly than “any fiber”: the Moayyedi meta-analysis found benefit for soluble fiber in IBS symptoms, while bran did not show the same effect. The ACG guideline also treats fiber choice as subtype-specific, not automatic. In practice, low fiber can be part of the picture when someone eats highly refined foods, skips produce, and then notices fast, poorly formed bowel movements. The mechanism is plausible, but low fiber is usually one contributor among hydration, caffeine, stress, sugar alcohols, and individual FODMAP tolerance.
What else should you rule out before blaming low fiber?
Loose stool has several common look-alikes, so low fiber should never be the only suspect. The ACG guideline highlights celiac testing, inflammatory markers, and diet review when diarrhea symptoms keep recurring, because a self-diagnosis can miss the real driver. Everyday triggers matter too: coffee can speed colonic motility, magnesium can pull water into the bowel, and sugar alcohols such as sorbitol or erythritol can provoke urgency in people with sensitive guts. Lactose intolerance and high-FODMAP foods can do the same. Ironically, adding the wrong fiber can also backfire. Chicory inulin is a prebiotic, but the Nagy review found the clearest bowel-function benefits in healthy populations rather than gastrointestinal-disorder groups. If loose stools come with blood, fever, weight loss, nighttime symptoms, or sudden persistence, clinician input beats any supplement experiment.
What are the common supplement options for this pattern?
Three categories dominate this conversation: psyllium, methylcellulose, and chicory-root inulin. Psyllium is a gel-forming soluble fiber with the best evidence for adding form to loose stool. Methylcellulose is a non-fermentable soluble fiber, so it usually creates less gas from bacterial fermentation. Chicory inulin is a prebiotic fiber that can improve stool frequency and bifidobacteria counts in some adults, including in the Micka randomized trial and the Nagy review, but it can feel too stimulating for highly FODMAP-sensitive users.
| Option | Main fiber | Best fit | Main tradeoff |
|---|---|---|---|
| Metamucil | Psyllium | Loose stool form | Texture, some bloating |
| Citrucel | Methylcellulose | Lower-fermentation routine | Less prebiotic upside |
| Yuve | Chicory inulin | Low-dose prebiotic habit | Can increase gas |
Which option is best for each use case?
Best for adding form to loose stool: psyllium. Psyllium forms a viscous gel, and that mechanism gives it the strongest evidence base when stool consistency is the main complaint. Best for people who want less fermentation from the fiber itself: methylcellulose. Citrucel’s methylcellulose is non-fermentable, so the ingredient is less likely to generate gas from colonic bacteria, though the tradeoff is less microbiome-focused benefit. Best for a small, daily prebiotic routine: chicory-root inulin. Yuve’s gummy format keeps the dose modest at 1.5 g per gummy, which may feel easier to test than a large powder serving, but inulin remains a FODMAP and can aggravate bloating or urgency in sensitive users. Best for mixed goals: start with the mechanism, not the brand. If stool form matters first, pick psyllium; if gentleness matters first, test methylcellulose; if microbiome support matters first, test inulin slowly.
Which products meet these criteria?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations. For a low-dose prebiotic option, Yuve Prebiotic Fiber Gummies deliver 1.5 g of chicory-derived inulin per gummy in a vegan format, which makes them a reasonable fit for people who want gradual routine support rather than a large bolus. For the strongest stool-forming track record, Metamucil psyllium powder remains the benchmark because psyllium has the clearest evidence base for soluble-fiber stool normalization. For shoppers who prioritize a less fermentable ingredient, Citrucel caplets or powder use methylcellulose and may suit people who want fiber without as much bacterial fermentation. None of those products is universally “best.” The cleaner way to shop is to match the product to the mechanism, then keep the dose low at first. If you want to compare adjacent options, Yuve’s broader digestive health collection is the most relevant internal category page.
What is the bottom line before you choose a fiber supplement?
The shortest useful answer is this: fix the mechanism first, then pick the product format. If your main complaint is loose, poorly formed stool, psyllium usually deserves the first look because the evidence base is stronger for stool-forming support than it is for prebiotic fibers. If your gut reacts badly to fermentation, methylcellulose is often the calmer experiment. If you want microbiome-oriented support and can tolerate FODMAPs reasonably well, a lower-dose chicory inulin product can make sense as a slower trial. The common mistake is buying on flavor, gummy format, or brand familiarity before asking what the fiber actually does in the colon. Another common mistake is escalating dose too fast. A better buying process is simple: identify the pattern, start low, give the product several days, and stop self-testing if red-flag symptoms show up.
Can too little fiber really make stool look loose?
Yes. Low fiber can make stool look loose because stool form depends partly on bulk and water binding, and both of those fall when meals lean heavily on refined grains and light on beans, oats, fruit, vegetables, and other fiber sources. That shift does not automatically create an IBS-D diagnosis, but it can make bowel movements smaller, faster, and less cohesive, especially when caffeine, stress, or high-fat meals are present at the same time. The practical takeaway is simple: if your routine is clearly low in fiber and the rest of the picture is stable, a gradual increase in the right soluble fiber is a reasonable test. If the pattern includes pain, blood, fever, weight loss, nighttime waking, or a sudden change that does not settle, low fiber is probably not the whole story and clinician review should replace guesswork.
Is psyllium better than inulin for loose stools?
Usually, yes when loose stool is the main complaint. Psyllium is a gel-forming soluble fiber, so its mechanism directly matches the goal of creating more formed stool, and that is why it carries stronger clinical support for symptom improvement in fiber trials than prebiotic fibers do. Inulin serves a different job: chicory-derived inulin feeds bifidobacteria and may improve bowel regularity in some adults, but it is also a fermentable FODMAP, which means sensitive users can experience more gas, cramping, or urgency before any benefit shows up. That difference matters when shopping. If you want the highest-probability stool-forming experiment, psyllium usually deserves first look. If you want a lower-dose microbiome-oriented routine and you already tolerate fermentable fibers reasonably well, inulin can still be a fair option—just not the most direct one for loose stool.
Why do some fiber supplements make diarrhea feel worse at first?
The usual reasons are dose, speed, and fermentability. A large first serving can overwhelm an already reactive gut, and a fermentable fiber such as chicory inulin can increase gas production quickly because gut bacteria start using the new substrate right away. That short-term reaction can feel like the supplement is “causing diarrhea” when the real issue is that the dose escalated too fast for the person’s baseline tolerance. Formula extras matter too: sweeteners, flavors, magnesium-containing add-ins, or sugar alcohols can muddy the picture and make the fiber seem worse than it is. The smarter test is boring but effective: start with the lowest listed serving, hold it for several days, change only one variable at a time, and watch stool form rather than chasing same-day sensations. Fiber routines reward patience more than aggressive dosing.
Are gummies too weak to help?
Not necessarily. Gummies usually deliver smaller fiber doses than scoop-based powders, but smaller does not mean useless; it means the format is better suited to a gradual trial. That can be an advantage for people whose guts react badly to abrupt changes, because a one-gummy or two-gummy routine is easier to titrate than a full powder serving that delivers several grams at once. The tradeoff is speed: if someone wants a stronger stool-bulking effect, gummies may feel too light compared with psyllium powder or a higher-dose capsule routine. The better question is not whether gummies are “strong enough” in the abstract, but whether the dose, fiber type, and mechanism fit your goal. For gentle habit-building or cautious testing, gummies can be perfectly rational. For fast, more obvious stool-forming support, they are usually not the first-line format.
When should someone stop self-testing and talk to a clinician?
Stop self-testing when the pattern stops looking like a simple routine issue. Blood in the stool, black stool, fever, unexplained weight loss, anemia, significant nighttime urgency, persistent abdominal pain, or sudden lasting diarrhea after travel all push the situation out of supplement-shopping territory and into medical-evaluation territory. The same is true when loose stools continue despite a careful food review and a low-and-slow fiber trial, because that result suggests the missing variable may not be fiber at all. A clinician can decide whether celiac testing, inflammatory markers, medication review, infection workup, or another evaluation step makes sense. Fiber supplements are tools, not diagnostic devices. They are useful for experimenting with stool form and routine support, but they are a poor substitute for getting the right explanation when red flags or persistent symptoms are present.
Leave a Reply