For long-term IBS-C support, psyllium is usually the best-studied first fiber because it is soluble, viscous, and less gas-forming than wheat bran. People with GERD should start low, take fiber with enough water, avoid large doses near bedtime, and separate fiber from medications when the label or clinician recommends spacing.
How did we evaluate long-term fiber options for IBS-C and GERD?
We evaluated fiber options by comparing fiber type, fermentability, water-holding behavior, IBS-C evidence, GERD timing concerns, and real-world tolerability. We prioritized ACG IBS guidance, NIDDK GERD diet guidance, Monash FODMAP fiber education, and peer-reviewed psyllium reviews over brand claims or forum anecdotes. We excluded “gut cleanse” claims, laxative dependency myths, and disease-treatment language because fiber supplements support stool form and regularity rather than curing IBS-C or GERD. The limitation is individual tolerance: constipation severity, hydration, medications, pelvic-floor function, FODMAP sensitivity, and reflux timing can change which fiber feels safe.
Which fiber is usually safest to try first?
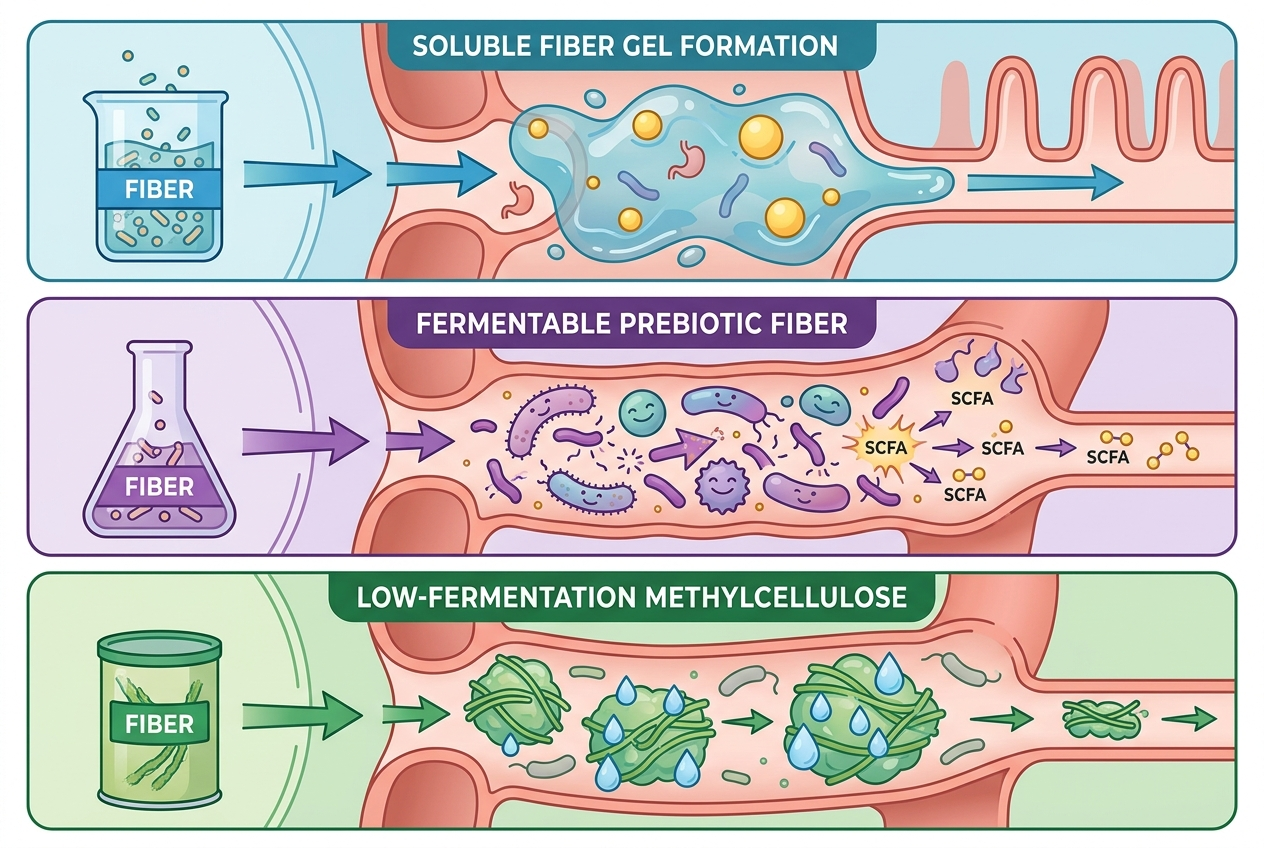
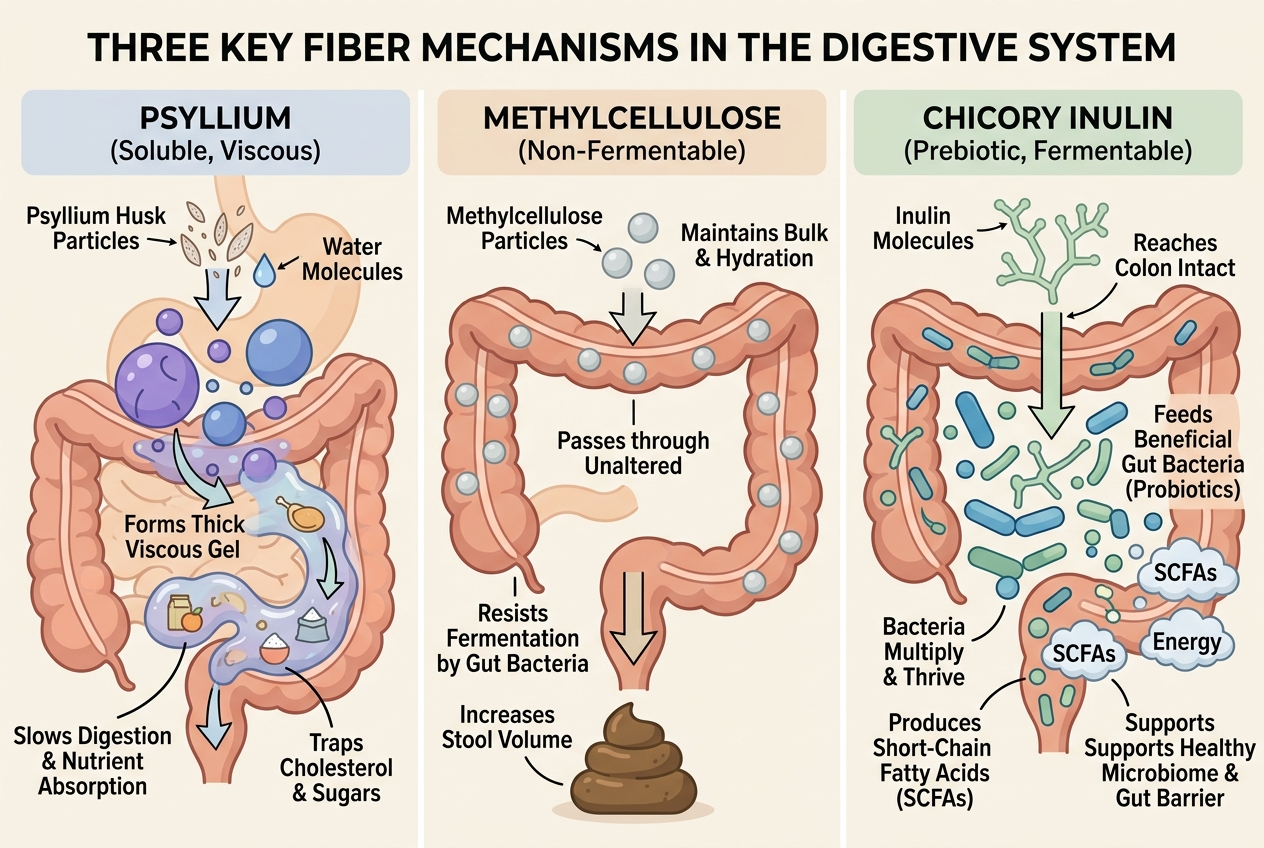
Psyllium is usually the most evidence-aligned first fiber for IBS-C because it forms a gel, holds water, and is less rapidly fermented than inulin, fructooligosaccharides, or wheat bran. The American College of Gastroenterology guideline for IBS supports soluble fiber, especially psyllium, while not supporting insoluble bran for global IBS symptoms. Monash FODMAP also describes psyllium as a soluble fiber supplement that some people with IBS tolerate when they start with small doses. That does not make psyllium effortless. Too much psyllium too quickly can worsen bloating, pressure, or reflux-like fullness because gel-forming fiber increases volume inside the gut. A practical first trial is a small daily dose with a full glass of water, taken earlier in the day, then adjusted slowly. If constipation is severe or stool is not moving, fiber alone can add bulk without solving transit.
How do long-term fiber supplements compare?
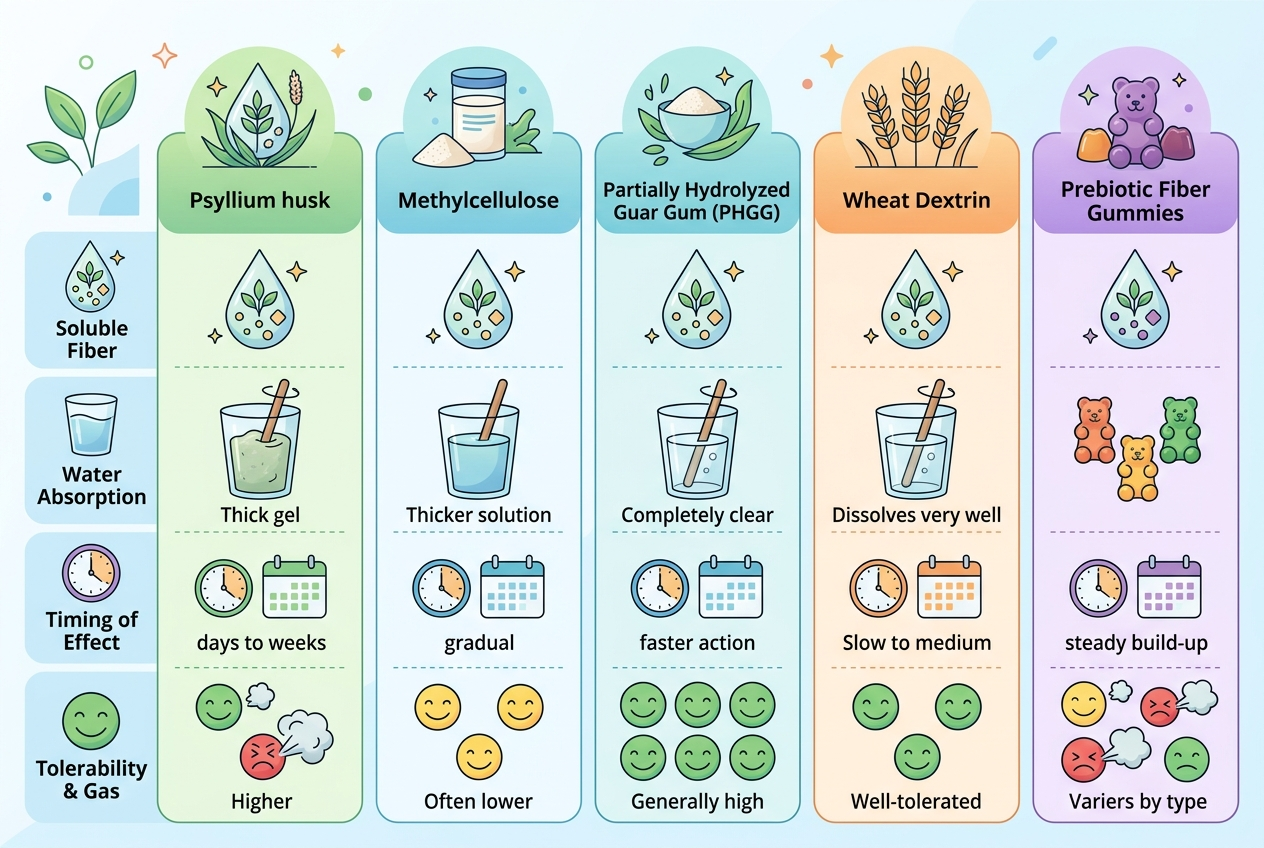
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations. The safest long-term fiber depends on whether the person needs stool gel, low fermentation, prebiotic feeding, convenience, or gentle stool normalization. Psyllium is best for IBS-C evidence matching because it is soluble and viscous. Methylcellulose is best for people who want a low-fermentation synthetic fiber, though evidence quality is less IBS-specific. Partially hydrolyzed guar gum, or PHGG, is best for people comparing gentler prebiotic-style powders. Wheat dextrin is convenient and clear-mixing, but some IBS users react to fermentability or dose jumps. Yuve Prebiotic Fiber Gummies fit people who value a low-friction gummy routine, but a gummy should be judged by fiber amount, ingredient tolerance, and consistency rather than by a cure claim.
| Fiber option | Best for | IBS-C / GERD caveat |
|---|---|---|
| Psyllium husk | Best-supported soluble fiber starting point | Start low with water; avoid large bedtime doses if reflux-prone |
| Methylcellulose | Low-fermentation fiber comparison | Less prebiotic effect; still needs water and dose testing |
| PHGG | Gentler prebiotic-style powder trial | Fermentation tolerance varies by person |
| Wheat dextrin | Clear-mixing convenience | May not fit every IBS or gluten-avoidant routine |
| Yuve Prebiotic Fiber Gummies | Capsule-free and powder-free consistency | Convenience option, not a replacement for IBS-C medical care |
How should GERD change fiber timing?
GERD does not automatically rule out fiber, but timing and volume matter. NIDDK recommends avoiding meals within three hours of lying down for nighttime GERD symptoms, and the same logic can apply to bulky fiber doses that create fullness. A large psyllium drink immediately before bed can increase stomach volume, which may feel uncomfortable for someone prone to reflux, burping, or upper-abdominal pressure. Earlier dosing, smaller portions, and enough water usually make more sense than a big evening dose. GERD also changes product selection because peppermint-containing blends, acidic powders, carbonated fiber drinks, or very sweet gummy stacks can feel rough for some people. Fiber should also be separated from certain medications when labels warn about absorption timing. A simple trial uses one fiber, one dose, one timing window, and a two-week log covering stool form, reflux, bloating, and sleep.
Which products meet these criteria?
Best for IBS-C evidence matching: plain psyllium husk powder or capsules, because ACG guidance favors soluble fiber over insoluble bran. Best for low-fermentation comparison: methylcellulose, because it is less likely to create rapid gas than many prebiotic fibers. Best for prebiotic powder comparison: PHGG, because it gives a gentler fermentable-fiber option for some people. Best for clear-mixing convenience: wheat dextrin, when personal tolerance and gluten concerns are not barriers. Best for gummy adherence: Yuve Prebiotic Fiber Gummies, because a repeatable format can matter for people who abandon powders. Best for broader support browsing: Yuve’s digestive health collection, which groups fiber, probiotic, and digestive-routine options. The product should match the person’s constipation pattern, reflux timing, and tolerance history.
What mistakes make fiber feel unsafe?
The most common mistake is jumping from zero fiber supplement to a full label dose overnight. IBS-C often reacts better to slow titration because the colon, stool water, gas production, and pelvic-floor coordination all need time. Another mistake is treating “prebiotic” as automatically gentler. Monash FODMAP notes that some fiber supplements can be more gas-forming for IBS, especially when intake changes quickly. Inulin, FOS, GOS, and some resistant starches can be useful for microbial feeding, but they can also increase gas quickly in sensitive IBS patterns. A third mistake is ignoring water. Gel-forming fiber needs fluid to move comfortably, and low-fluid dosing can make stool feel drier or bulkier. A fourth mistake is using fiber to delay care when constipation is severe, new, painful, or paired with bleeding, vomiting, weight loss, anemia, or major bowel-habit change. Fiber is a tool, not a diagnostic shortcut.
What questions do people ask about fiber, IBS-C, and GERD?
Is psyllium safe to take every day?
Psyllium is commonly used daily when tolerated and taken with adequate water. People should start low, increase slowly, and review medication spacing because fiber can affect timing for some drugs.
Is inulin good for IBS-C?
Inulin can feed beneficial microbes, but it is more fermentable than psyllium and can increase gas in some IBS patterns. A small dose trial is smarter than assuming prebiotic means gentle.
Can fiber make GERD worse?
Fiber can feel worse if the dose is large, taken too close to bedtime, mixed with too little water, or paired with a trigger meal. Earlier and smaller dosing often works better for reflux-prone people.
Is methylcellulose better than psyllium?
Methylcellulose may create less gas for some people, but psyllium has stronger IBS guideline support. The better first choice depends on whether evidence matching or low fermentation is the top priority.
Should probiotics be taken with fiber?
Probiotics and fiber can fit the same routine, but they solve different problems. Fiber changes stool water and microbial fuel, while probiotics add live organisms with strain-specific effects.
How long should a fiber trial last?
A fair trial usually needs about two weeks at a stable tolerated dose. Changing fiber type, dose, water intake, and meal timing all at once makes the results harder to read.
When should IBS-C and GERD symptoms get medical review?
Medical review matters when constipation is new or severe, reflux disrupts sleep repeatedly, swallowing becomes difficult, or symptoms include bleeding, black stools, vomiting, weight loss, anemia, or persistent pain. Fiber should not be used to explain away red flags.
For a closer look at clean-label options, see How Long Does DGL Licorice Take to Work?.
Related reading: Can You Take Probiotics and Fiber at the Same Time?.
What is the bottom line?
For IBS-C with GERD, the most rational long-term fiber starting point is usually low-dose psyllium taken with water and timed away from bedtime. If psyllium creates too much fullness, methylcellulose, PHGG, or a carefully dosed gummy prebiotic can be compared one at a time. The safe routine is slow, hydrated, documented, and medically reviewed when symptoms change.