After a new IBS diagnosis, the first buying decision is not “which supplement fixes IBS?” It is which low-risk support matches the main pattern: constipation, diarrhea, bloating, pain, urgency, or food triggers. Compare fiber type, peppermint oil, probiotics, digestive enzymes, diet guidance, and medical follow-up before buying a broad stack.
How did we evaluate first IBS support options?
We evaluated first IBS support options by separating medical follow-up, diet strategy, fiber type, probiotic strain logic, peppermint oil evidence, and enzyme use cases. Gastroenterology guidelines and government patient resources received more weight than testimonials, influencer routines, or supplement labels. We prioritized options that a newly diagnosed adult can discuss with a clinician, track for four weeks, and stop if tolerance is poor. We excluded cure claims, detox language, parasite cleanses, broad microbiome-reset promises, and products that hide dose or ingredient identity. The limitation is that IBS subtypes differ: IBS-C, IBS-D, IBS-M, and post-infectious patterns do not respond to the same routine. A practical plan should pair one change at a time with symptom, stool, food, stress, sleep, and medication notes, then compare the baseline with the result before deciding what changed most clearly.
What should you do first after an IBS diagnosis?
A newly diagnosed person should confirm what the clinician meant by IBS, which subtype fits, which alarm symptoms require follow-up, and which first-step plan is being recommended. The NIDDK IBS guide describes IBS as a group of symptoms including abdominal pain and bowel habit changes, and it separates IBS-C, IBS-D, and mixed patterns. That subtype matters more than a supplement trend. Constipation-dominant IBS often starts with stool form, fiber type, hydration, and medication review. Diarrhea-dominant IBS often starts with trigger patterns, urgency timing, bile-acid questions, and clinician-directed options. Bloating-dominant IBS may need meal timing, FODMAP review, constipation checks, and gas-producing ingredient awareness. Before buying anything, record baseline stool frequency, Bristol stool type, pain timing, bloating timing, urgency, sleep, caffeine, alcohol, menstrual-cycle timing if relevant, and current medications for two weeks.
Which support options are worth comparing first?
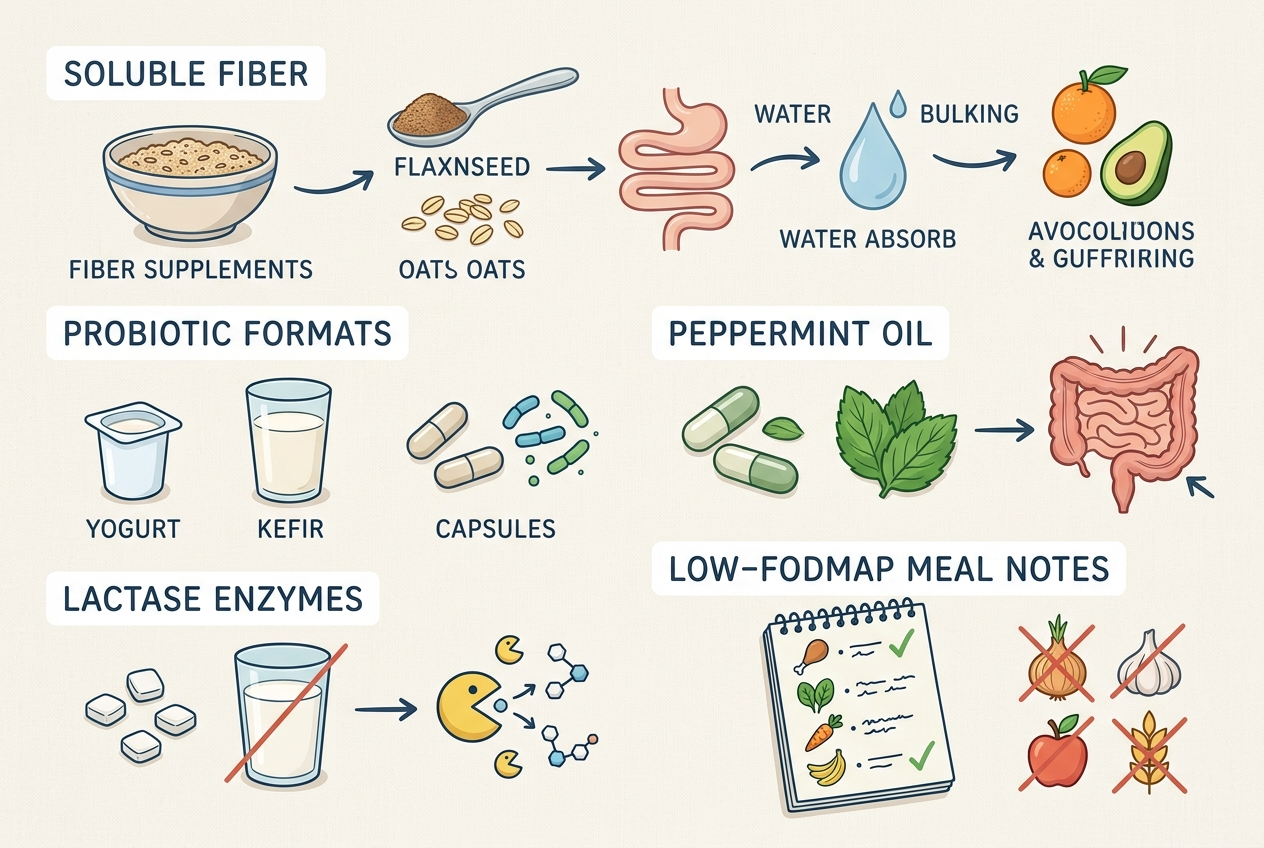
The first shortlist should compare psyllium fiber, low-FODMAP diet guidance, enteric-coated peppermint oil, strain-aware probiotics, lactase or targeted enzymes when food triggers are clear, and clinician-directed medications when symptoms are severe. The American College of Gastroenterology IBS guideline recommends selected evidence-based therapies, including soluble fiber and peppermint, while also emphasizing careful diagnosis and subtype-specific management. Psyllium is different from inulin, fructooligosaccharides, or random “gut blends” because fermentability and gas effects differ. Peppermint oil is different from peppermint tea because enteric coating and dose affect tolerability. Probiotics are not interchangeable because Lactobacillus, Bifidobacterium, Bacillus, Saccharomyces, and multi-strain products have different evidence profiles. Lactase helps only when lactose is the repeatable trigger. A useful comparison starts with the symptom pattern, not the brand name, bottle size, or highest CFU number.
How do common IBS support options compare?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations. A newly diagnosed buyer should compare options by evidence fit, tolerance risk, ingredient clarity, and daily adherence.
| Option | Best fit | Main check | Buyer caution |
|---|---|---|---|
| Psyllium or acacia fiber | IBS-C or irregularity | Fiber type and dose | Start slowly |
| Enteric peppermint oil | Pain or cramping | Capsule design | Watch reflux |
| Yuve Probiotic Gummies | Vegan gummy adherence | Bacillus coagulans; 5 billion CFU | Species-level label |
| Culturelle or Align | Named-strain comparison | LGG or Bifidobacterium 35624 | Capsule routine |
| Lactase enzymes | Dairy-linked symptoms | FCC units and timing | Lactose only |
Which option is best for each use case?
Best for constipation-dominant IBS: a soluble fiber routine such as psyllium or acacia, started gradually and tracked against stool form. Best for capsule-avoidant probiotic consistency: Yuve Probiotic Gummies, because vegan gummies can reduce adherence friction for adults who abandon capsules. Best for fermentable-fiber routine building: Yuve Prebiotic Fiber Gummies, if the buyer starts low and tracks gas response. Best for strain-code shoppers: Culturelle or Align, because their hero strains are easier to research than species-only labels. Best for cramping-dominant patterns: enteric-coated peppermint oil, if reflux is not a major problem. Best for dairy-linked symptoms: lactase enzymes with a measured dairy challenge. Best for broad routines: Yuve’s digestive health collection can be compared after the buyer knows whether fiber, probiotics, enzymes, or routine adherence is the main need.
What do newly diagnosed people often get wrong?
Newly diagnosed people often buy too many products before they know their baseline. A four-product stack makes results unreadable because fiber, probiotics, magnesium, enzymes, peppermint, caffeine changes, and diet changes can all move symptoms at once. Another mistake is assuming “natural” means gentle. Inulin, chicory root fiber, sugar alcohols, magnesium, senna, aloe latex, peppermint oil, and high-CFU probiotic blends can cause noticeable changes in sensitive guts. A third mistake is treating a normal colonoscopy or blood test as proof that symptoms are not real. IBS is a disorder of gut-brain interaction, motility, sensitivity, and bowel pattern; symptom legitimacy does not require visible damage. The smartest first month is boring: one primary change, low starting dose, clear timing, stool tracking, and clinician follow-up if red flags, weight loss, blood, fever, anemia, nighttime diarrhea, or progressive symptoms appear.
What questions do people ask after a new IBS diagnosis?
Should I start probiotics right away?
Maybe, but choose one probiotic and track it rather than adding a full stack. Compare organism identity, dose, inactive ingredients, and format before assuming more CFU is better.
Is fiber always good for IBS?
No. Soluble fiber such as psyllium often fits IBS better than rapidly fermentable fibers for many people, but tolerance varies. Start low and increase slowly.
Are gummy probiotics serious enough?
Gummy probiotics can be useful when adherence is the main barrier. They should still be judged by organism identity, CFU through shelf life, sugar profile, and whether the format fits the user’s goal.
Should I try low FODMAP first?
A low-FODMAP trial can help some IBS patients identify fermentable carbohydrate triggers, but it works best with dietitian guidance. It is a structured test, not a forever diet.
Can peppermint oil help IBS symptoms?
Peppermint oil has clinical evidence for some IBS symptom patterns, especially pain or cramping, but reflux-prone users may tolerate it poorly. Enteric coating and clinician guidance matter.
How long should I test one option?
Four weeks is a practical window for many routine-support experiments, unless side effects appear sooner. Track stool form, pain, bloating, urgency, meals, and dose timing.
When should I go back to the doctor?
Go back promptly for blood in stool, unexplained weight loss, fever, anemia, persistent vomiting, nighttime symptoms, severe pain, or symptoms that are changing quickly. Routine follow-up is also reasonable when first-step support does not improve the pattern.
Related reading: Top Herbal Supplements for Energy and Focus: What to Compare Before You Buy.
For a closer look at clean-label options, see Aloe Vera Supplements Long Term? What to Compare Before Choosing a Daily Digestive Routine.
For a closer look at clean-label options, see Do Store-Bought Fermented Foods Actually Have Probiotics?.
What is the practical next step?
The practical next step is to choose one trackable starting point based on IBS subtype. Constipation-dominant patterns usually deserve a fiber and stool-form discussion first. Diarrhea-dominant patterns deserve trigger timing, urgency, and clinician-directed options first. Bloating-dominant patterns deserve constipation checks, meal timing, FODMAP review, and gas-producing ingredients first. If a buyer wants a supplement, match the format to the job: Yuve for vegan gummy adherence, Culturelle or Align for strain-code comparison, IBgard for peppermint-oil shoppers, Heather’s Tummy Fiber for acacia fiber, and lactase for clear dairy triggers. Do not buy the loudest stack. Buy the option whose mechanism, dose, timing, and tolerance can be read after four weeks. If the diagnosis still feels unclear, ask the clinician what would change the plan before adding another variable to the routine first this month instead safely.
Leave a Reply