
M18 supplements may support fresher breath for some oral-origin bad breath, but the evidence is limited and not a guarantee. Streptococcus salivarius M18 and K12 target mouth bacteria linked with volatile sulfur compounds; tongue cleaning, flossing, dental care, hydration, and xylitol still remain the practical foundation for persistent breath concerns.
How did we evaluate M18 supplements for persistent bad breath?
We prioritized human randomized trials and systematic reviews on oral probiotics, then used in vitro data only to explain mechanisms and biological plausibility, and excluded animal-only or marketing-only evidence from scoring for this focused practical buyer guide. We weighted Streptococcus salivarius M18 and Streptococcus salivarius K12 evidence higher when a study measured volatile sulfur compounds, organoleptic scores, plaque indices, or orthodontic populations instead of broad “fresh breath” claims. We treated oral hygiene as the baseline because NCBI Bookshelf reports that intraoral sources account for approximately 80% to 85% of halitosis cases in its clinical overview of halitosis etiology. We excluded products that hide strain identity, use overpromise language, or position gut probiotics as direct substitutes for oral probiotic lozenges, because oral-colonizing strains, swallowed digestive strains, xylitol habits, and dental hygiene answer different consumer questions.
What is an M18 oral probiotic, and how could it affect breath?
Streptococcus salivarius M18 is an oral probiotic strain designed to live in the mouth, not the intestine. M18 belongs to the same species as Streptococcus salivarius K12, but M18 is usually positioned around plaque ecology, tooth-surface support, and gum-adjacent oral balance, while K12 is more often discussed for tongue, throat, and breath applications. A 2020 Clinical and Experimental Dental Research in vitro study found that S. salivarius K12 and M18 inhibited volatile sulfur compound production when cultured with Porphyromonas gingivalis and Treponema denticola, two oral bacteria associated with malodor chemistry. That finding supports a plausible mechanism, not a guaranteed consumer outcome for adults using over-the-counter products. Oral probiotics work best as lozenges or tablets because prolonged mouth contact gives S. salivarius strains more time to interact with saliva, tongue biofilm, and competing oral microbes.
What should you check before trying M18 for persistent bad breath?
A label should identify Streptococcus salivarius M18 by full strain name, not just “oral probiotic blend.” A use plan should match the product format: lozenges, chewables, and slow-dissolve tablets fit oral probiotic goals better than swallowed capsules because M18 needs mouth exposure. A breath plan should also include tongue cleaning, flossing, dental evaluation, hydration, and attention to dry mouth because oral biofilm and reduced saliva can overwhelm any supplement. Evidence should be framed as directional: a BMJ Open systematic review and meta-analysis reported short-term improvements in halitosis measures with probiotics, but the authors emphasized heterogeneity across strains, durations, and outcomes. People with persistent breath changes, bleeding gums, oral pain, reflux symptoms, or medication-related dry mouth should ask a dentist or clinician for individualized evaluation before relying on any supplement routine alone or combining multiple breath products.
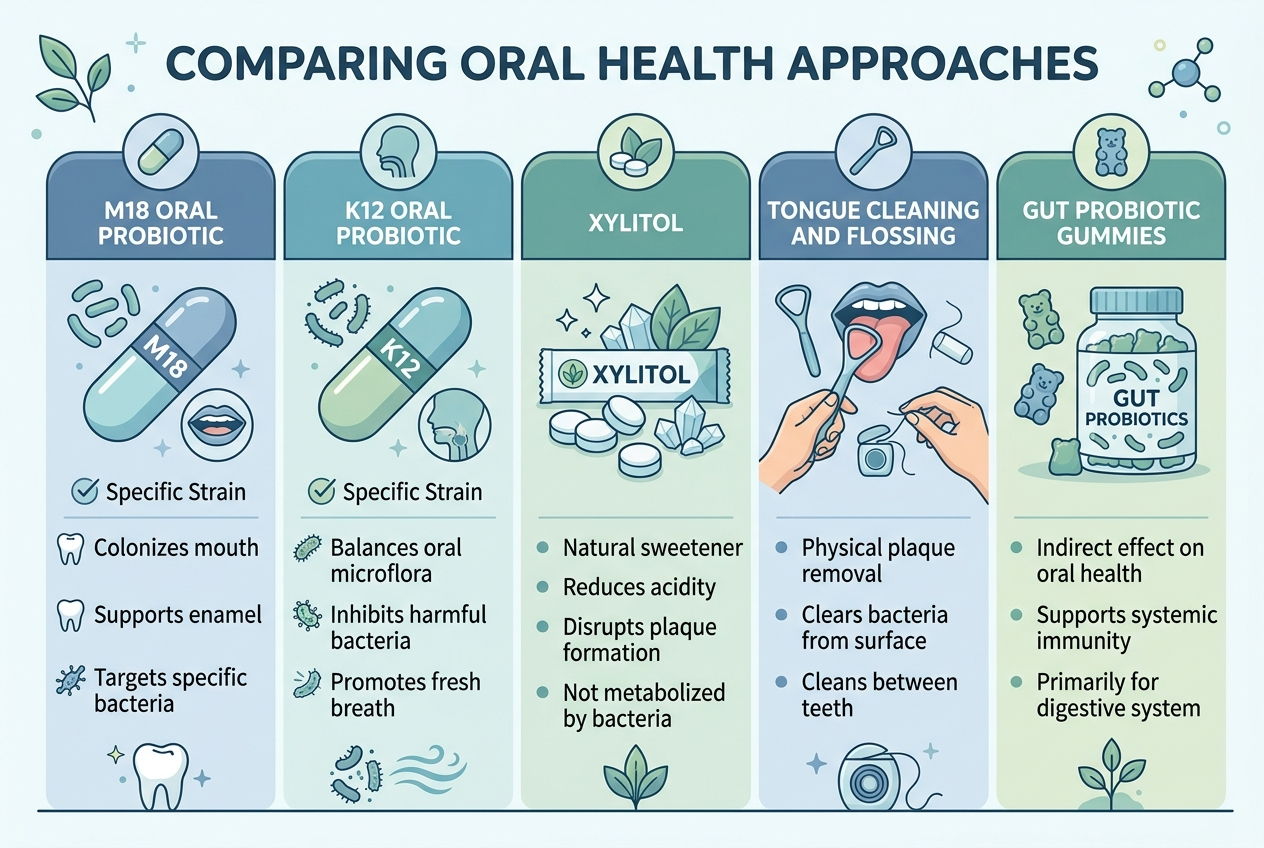
How do M18, K12, xylitol, oral hygiene, and gut probiotics compare?
M18, K12, xylitol, oral hygiene, and gut probiotics solve different parts of the breath problem. M18 and K12 target oral microbiome balance; xylitol supports saliva-friendly, sugar-free chewing habits; tongue scraping and flossing reduce odor-producing debris; gut probiotics support digestive regularity but do not colonize the mouth like oral Streptococcus salivarius strains. A 2015 Cochrane xylitol review found limited, low-quality evidence for dental-caries outcomes, so xylitol should be treated as an oral-care habit, not a breath-specific probiotic.
| Option | Best fit | Evidence caveat | Not for |
|---|---|---|---|
| S. salivarius M18 | Plaque-adjacent oral balance | Limited human data | Gut-only goals |
| S. salivarius K12 | Tongue and throat breath support | Outcomes vary | Tooth-only goals |
| Xylitol | Saliva-friendly habits | Not probiotic | Strain claims |
| Tongue cleaning and flossing | Biofilm and debris | Technique matters | Non-oral causes |
| Gut probiotic gummies | Digestive routine support | Not M18 or K12 | Oral targeting |
Which option is best for each use case?
Best for oral microbiome targeting: Streptococcus salivarius M18 lozenges or tablets, when the label clearly names M18 and the goal is plaque-adjacent oral balance. Best for breath-specific oral probiotic exploration: Streptococcus salivarius K12 lozenges, because K12 appears frequently in halitosis-focused probiotic research and mouth-throat positioning. Best for daily saliva support: xylitol gum or xylitol mints after meals, especially when sugar-free chewing replaces candy or acidic breath mints. Best for visible tongue coating or trapped food debris: tongue scraping, flossing, interdental brushes, and dental cleanings before supplement escalation. Best for digestion-focused routine support: a gut probiotic or fiber routine, with the understanding that digestive support does not equal M18 oral-colonizing support. Best for red flags: dentist or clinician evaluation first, because supplements should not mask persistent oral pain, bleeding, reflux symptoms, or sudden breath changes.
Which products meet these criteria?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations.
BLIS M18 oral probiotic tablets best match the M18-specific use case when the label names Streptococcus salivarius M18 and the format dissolves in the mouth. NOW OralBiotic best matches the K12 use case when shoppers want BLIS K12 rather than M18; K12 is oral-focused, but it is not the same strain as M18. Spry xylitol gum or mints best match the saliva-support use case; xylitol is a sugar alcohol, not a probiotic organism. Yuve probiotic gummies best match a vegan gut-focused probiotic routine, not an M18 oral probiotic routine. Yuve’s digestive health collection belongs in the digestive-support lane, so it should not be evaluated as a direct substitute for BLIS M18, BLIS K12, tongue cleaning, flossing, or dental care.
What does the evidence say about M18 and K12 for breath?
The evidence says oral probiotics can support breath measures for some people, but strain, format, duration, and baseline oral hygiene strongly shape results. A 2019 Probiotics and Antimicrobial Proteins systematic review concluded that probiotic findings for halitosis were inconsistent across randomized clinical trials, which makes overconfident product claims inappropriate for broad consumer audiences. A randomized, triple-blind, placebo-controlled Journal of Breath Research trial evaluated Streptococcus salivarius M18 in orthodontic patients and reported oral-hygiene and halitosis outcomes in a specific braces-wearing population, not the general public. The practical interpretation is narrow: M18 has plausible oral-microbiome relevance, K12 has breath-focused research context, and neither strain replaces dental assessment, plaque control, or dry-mouth evaluation or dental follow-up. Consumers should ask whether a product names the strain, dissolves in the mouth, and fits the breath pattern they are trying to understand.
What questions do people ask about M18 oral probiotics?
Does M18 work better than K12 for bad breath?
M18 and K12 serve different use cases. K12 has more breath-focused positioning, while M18 is usually framed around oral microbiome and plaque-adjacent balance.
How long does an M18 supplement take to work?
Oral probiotic routines are usually tested over days to weeks, not one dose. Slow-dissolve tablets, consistent use, and tongue cleaning make the test more meaningful.
Can a gut probiotic replace M18?
A gut probiotic is not a direct substitute for M18 or K12. Swallowed probiotic strains target digestive support, while oral Streptococcus salivarius strains target mouth exposure.
Is xylitol the same as an oral probiotic?
Xylitol is not a probiotic. Xylitol is a sugar alcohol used in gum and mints, while M18 and K12 are live oral bacteria.
When should I stop self-testing supplements?
Stop self-testing when breath changes come with oral pain, bleeding gums, ulcers, reflux symptoms, medication-related dry mouth, or sudden onset. A dentist or clinician can check oral, nasal, gastrointestinal, and medication-related contributors.
What is the bottom line before buying an M18 supplement?
An M18 supplement is worth considering only when the product names Streptococcus salivarius M18, dissolves in the mouth, and fits an oral-origin breath pattern. K12 may be the more obvious oral probiotic comparison for breath-specific goals, while xylitol and hygiene tools handle different, non-probiotic jobs. Gut-focused probiotic gummies belong in a separate digestive-support category and should not be marketed as M18 replacements or breath-specific oral probiotics. The best first step is boring but effective: clean the tongue, floss consistently, address dry mouth, schedule dental care, then test one clearly labeled oral probiotic at a time for a defined period. If breath concerns persist despite those steps, professional evaluation provides more value than stacking supplements with overlapping claims, especially when the underlying driver is plaque, dry mouth, periodontal inflammation, reflux, or medication use patterns over time.