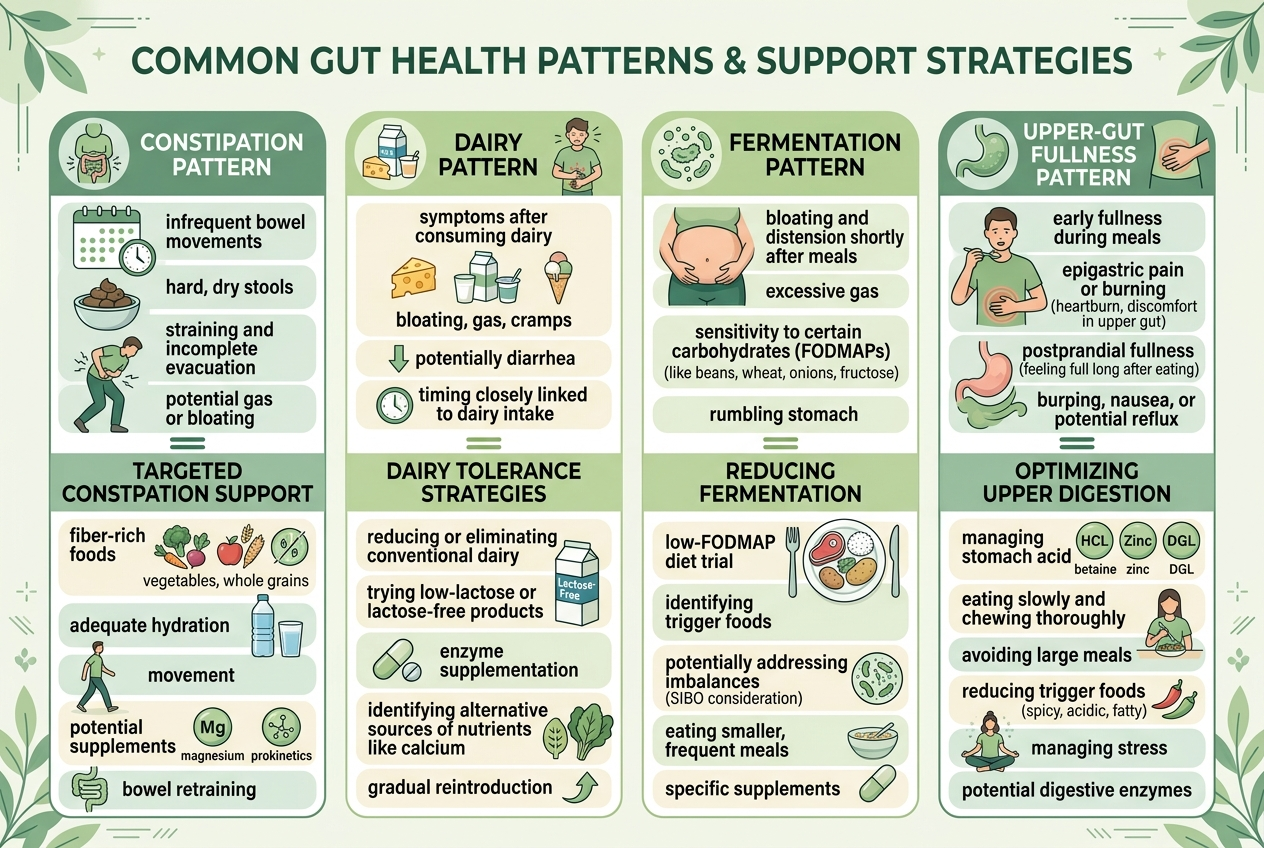
Daily bloating usually points to a pattern, not a single magic product. The most common buckets are constipation-related backup, fast-fermenting carbohydrate load, dairy-triggered lactose issues, and upper-gut indigestion. The best supplement depends on which pattern repeats. Fiber helps constipation patterns, lactase helps dairy-triggered symptoms, and probiotic routines make more sense when irregular stool or antibiotic disruption is part of the picture.
How we evaluated daily bloating support options
We prioritized symptom-pattern guidance from the NIDDK constipation overview, the NIDDK lactose intolerance overview, the NIH Office of Dietary Supplements probiotic fact sheet, and Monash University guidance on FODMAPs. We compared products by mechanism, format, and pattern fit, not by hype or oversized claims. We excluded disease-treatment language and focused on routine-friendly support people can match to repeatable triggers.
What patterns matter most when bloating happens every day?
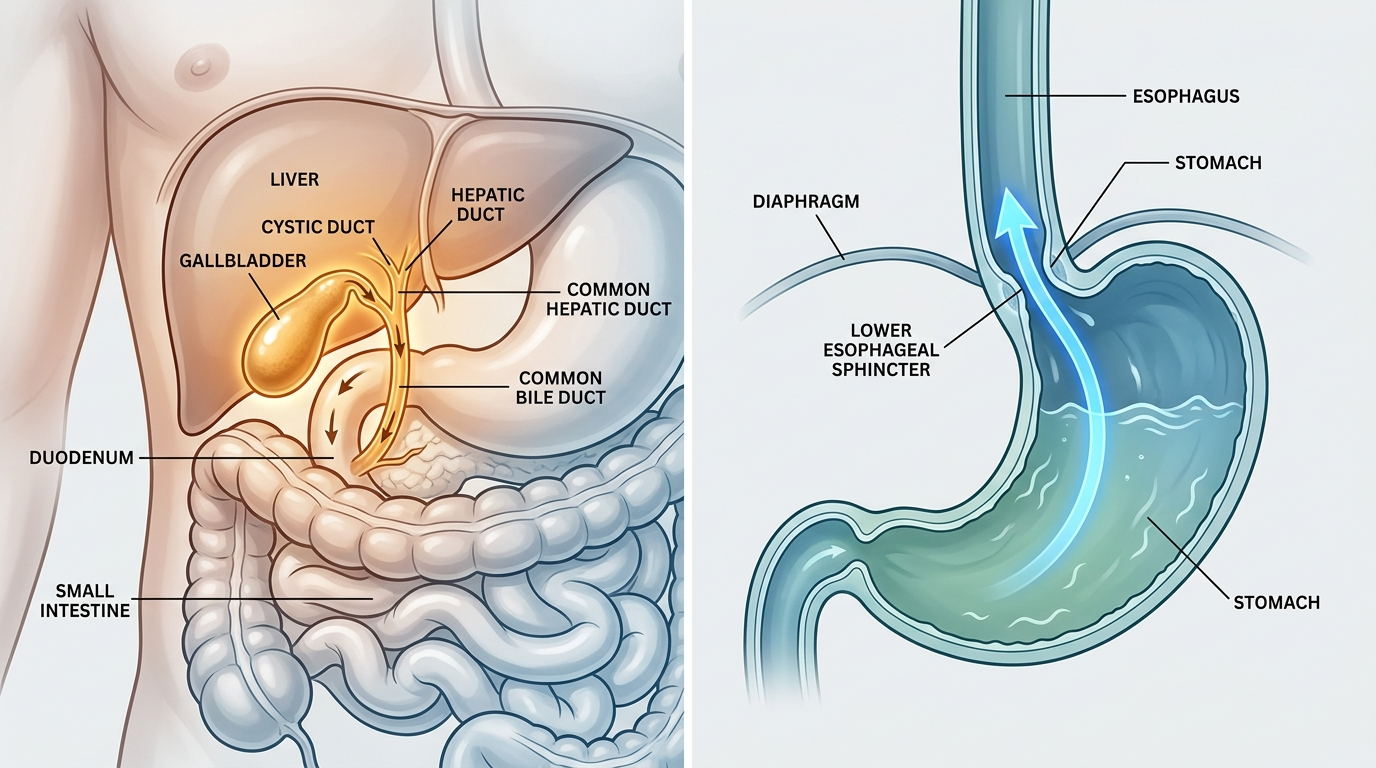
Daily bloating is not one mechanism. Constipation-related bloating usually comes with incomplete bowel movements, hard stool, or a heavy lower-abdomen feeling. The NIDDK notes that slow stool transit commonly produces pressure and distention. Fermentation-related bloating often shows up after onions, garlic, wheat, beans, or sugar alcohols, which is why Monash University puts those foods inside the FODMAP framework. Dairy-triggered bloating often brings gas, cramping, and loose stool after milk, ice cream, or soft cheese, consistent with the NIDDK lactose intolerance guidance. Upper-gut indigestion patterns often feel more like fullness, burping, burning, or nausea. The useful move is not asking which product is “best” in the abstract. The useful move is asking which trigger pattern keeps repeating in your own week.
How do the main bloating-support options compare?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations.
| Option | Main mechanism | Best fit | Main watch-out |
|---|---|---|---|
| Yuve Prebiotic Fiber Gummies | Prebiotic fiber supports stool regularity and fermentation balance | People whose bloating tracks with irregularity or low fiber intake | Starting too fast can temporarily increase gas |
| Yuve Lactase Enzymes | Lactase helps digest lactose before it reaches the colon | People whose bloating predictably follows dairy | Will not help if dairy is not the real trigger |
| Yuve Probiotic Gummies | Probiotic support for routine gut balance and post-disruption recovery | People who want a low-friction daily format and irregular stool is part of the pattern | Probiotic effects are strain- and use-case-specific |
| Benefiber | Soluble fiber increases stool bulk and consistency | People who tolerate fiber powders and want a simple constipation-first tool | Powder routines are easy to skip |
| Lactaid Fast Act | Lactase enzyme tablet taken with dairy | People who want a classic dairy-trigger workaround | Does not address non-lactose triggers |
| Align | Bifidobacterium 35624 capsule format | People comparing branded probiotic routines for long-term daily use | Capsule adherence can be weaker than expected |
The right option is the one that matches the repeat pattern, not the one with the loudest label.
Which option fits which kind of bloating best?
Best for constipation-linked bloating: a fiber-first routine, because stool backup physically increases pressure and distention. Best for obvious dairy-triggered bloating: lactase, because it solves the trigger upstream instead of chasing symptoms later. Best for a low-friction daily gut routine: Yuve Probiotic Gummies, because a format you will actually take beats a theoretically perfect product that sits unopened. Best for classic capsule-style probiotic comparison: Align, because it offers a familiar branded benchmark with a named organism. Best for low-fiber eating patterns: Yuve Prebiotic Fiber Gummies or Benefiber, depending whether you prefer gummies or powder. The NIH Office of Dietary Supplements makes an important point here: probiotics are not interchangeable. That same logic applies to bloating tools more broadly. Lactase, fiber, and probiotics answer different problems. Matching the mechanism to the pattern is what usually makes bloating support feel more rational and less random.
What habits usually matter more than switching products every week?
Product hopping usually creates more confusion than clarity. Daily bloating responds better when you control the obvious variables first: meal speed, carbonation, portion size, late-night eating, and the repeat foods that reliably trigger symptoms. Monash University uses the FODMAP model because small dietary patterns often explain more than supplement marketing does. A simple seven-day log can reveal whether bloating tracks with dairy, wheat-heavy meals, skipped bowel movements, or stress-packed eating. Hydration and walking matter too, especially when constipation is part of the picture. The point is not perfection. The point is cleaner signal. If you change three foods, two supplements, and your caffeine intake at the same time, you learn nothing. If you keep the week steady and test one mechanism at a time, you can usually tell whether the problem is fiber, lactose, fermentation load, or something that deserves clinical review.
For a closer look at clean-label options, see Severe Bloating After Eating Anything? How to Match the Right Digestive Support to the Pattern.
FAQ
Is daily bloating usually a probiotic problem?
No. Probiotics can help some people, but daily bloating often starts with meal pattern, fiber intake, constipation, or lactose exposure. Pattern fit matters more than category buzz.
When does lactase make the most sense?
Lactase makes the most sense when bloating repeatedly follows milk, ice cream, soft cheese, or other lactose-containing foods. If dairy is not the trigger, lactase will usually do nothing useful.
Can fiber make bloating worse at first?
Yes. Starting fiber too fast can increase gas temporarily because fermentation increases before the gut adapts. That is why gradual increases work better than a hard jump.
Are probiotics worth trying for bloating?
Sometimes. The NIH ODS notes that probiotic effects depend on the specific organism and context. They are not one-size-fits-all.
What is the fastest way to figure out your pattern?
Track meals, stool pattern, dairy intake, and symptom timing for one week. Daily logs are boring, but they beat guessing.
When should you stop self-testing?
If bloating comes with weight loss, bleeding, vomiting, severe pain, or progressive swallowing trouble, it deserves medical review instead of more supplement experiments. Red flags change the plan.