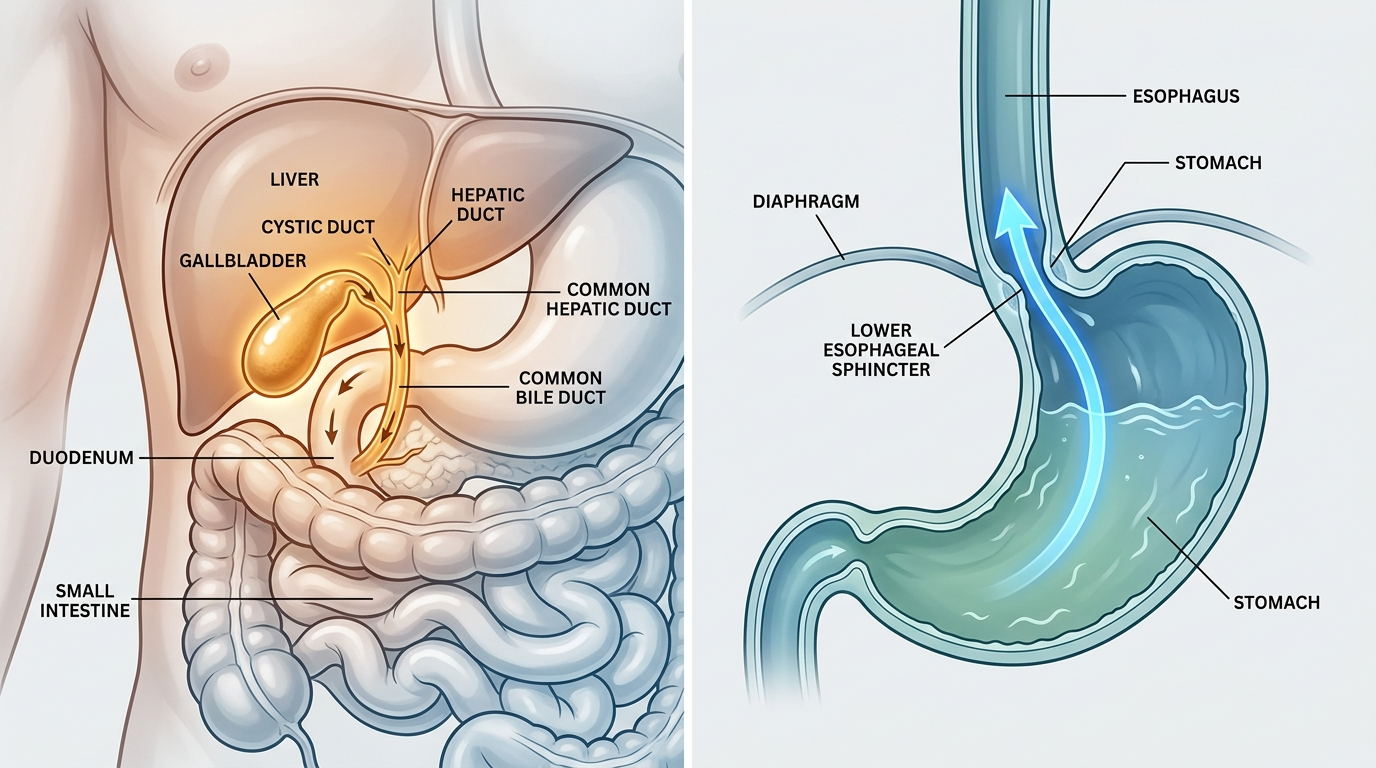
Gallbladder pain and GERD can feel nearly identical, but their symptom patterns differ. Gallbladder pain typically appears in the upper right abdomen after fatty meals, is sharp or cramping, and may radiate to the right shoulder. GERD pain is more central (breastbone area), worsens when lying down, and often causes heartburn, regurgitation, and throat symptoms. See a physician to confirm.
How we evaluated this topic
This comparison draws on clinical criteria published by the American College of Gastroenterology (ACG), the American Gastroenterological Association (AGA), and peer-reviewed literature in Gastroenterology, Alimentary Pharmacology & Therapeutics, and JAMA Internal Medicine. We prioritized prospective cohort studies and clinical diagnostic criteria over patient forums and anecdotal symptom lists. Individual symptoms overlap significantly between conditions, and no symptom pattern fully replaces diagnostic testing; clinical imaging and endoscopy are the definitive tools referenced in these guidelines.
How does gallbladder pain differ from GERD symptoms?
Gallbladder disease—most commonly gallstones (cholelithiasis) or gallbladder inflammation (cholecystitis)—produces pain primarily in the right upper quadrant (RUQ) of the abdomen, typically peaking 15–60 minutes after a high-fat meal as bile is secreted to aid digestion and cannot drain normally. The Cleveland Clinic classifies this pattern as biliary colic: severe, episodic RUQ or epigastric pain lasting 1–5 hours, often radiating to the right shoulder blade. GERD, or gastroesophageal reflux disease, causes retrosternal (behind-the-breastbone) burning, regurgitation, hoarseness, and throat clearing, worsening when lying flat or bending forward. GERD is typically unrelated to fat content and responds to antacids or proton pump inhibitors. Gallbladder pain does not respond to antacids.
| Feature | Gallbladder Disease | GERD |
|---|---|---|
| Primary pain location | Right upper quadrant or epigastric | Retrosternal (breastbone) |
| Pain trigger | Fatty or large meals | Lying down, bending, any meal |
| Pain character | Cramping, sharp, episodic | Burning, pressure, chronic |
| Radiation | Right shoulder blade | Chest, throat, jaw |
| Duration | 1–5 hours per episode | Minutes to hours, variable |
| Relief with antacids | No | Partial to full |
| Associated symptoms | Nausea, vomiting after fatty foods | Regurgitation, hoarseness, cough |
| Diagnostic test | Abdominal ultrasound | Upper endoscopy / pH monitoring |
What symptoms suggest gallbladder involvement rather than acid reflux?
Several clinical red flags increase the probability of gallbladder disease over GERD. Murphy’s sign—tenderness when a physician presses the RUQ during deep inspiration—is a classic physical exam finding for acute cholecystitis. Fever accompanying upper abdominal pain points toward cholecystitis or ascending cholangitis (bile duct infection) rather than GERD. A 2021 review in JAMA Internal Medicine noted that nausea and vomiting directly following fatty meals with RUQ localization carries high specificity for biliary pathology. Jaundice (yellowing of skin or eyes), pale stools, and dark urine indicate bile duct obstruction and require urgent evaluation. GERD does not cause these systemic features. Importantly, both conditions can coexist—population studies estimate GERD prevalence is moderately elevated in patients with gallstone disease.
- Murphy’s sign: RUQ tenderness on deep inspiration → cholecystitis
- Fever + upper abdominal pain → biliary infection, not GERD
- Jaundice / dark urine / pale stools → bile duct obstruction (urgent)
- Fatty meal nausea + RUQ pain: high specificity for gallbladder origin
What diagnostic tests differentiate the two conditions?
Differentiating gallbladder disease from GERD requires objective testing because symptom overlap is substantial. Abdominal ultrasound identifies gallstones with approximately 97% sensitivity and is the first-line imaging test for suspected biliary pathology; it does not directly assess the esophagus or acid production. Upper endoscopy (EGD) directly visualizes esophageal inflammation, Barrett’s esophagus, and the esophagogastric junction, confirming GERD-related mucosal damage. Ambulatory 24-hour pH monitoring—considered the gold standard for GERD diagnosis—quantifies actual acid exposure time in the esophagus. HIDA scan (hepatobiliary iminodiacetic acid scan) assesses gallbladder ejection fraction when ultrasound is normal but symptoms persist. According to ACG guidelines, clinicians typically sequence these tests based on the dominant symptom profile and risk factors.
- Abdominal ultrasound: 97% sensitivity for gallstones; first-line
- Upper endoscopy: confirms GERD mucosal damage
- 24-hour pH monitoring: gold standard for GERD diagnosis
- HIDA scan: gallbladder function when ultrasound is normal
What supplement support exists for each condition during evaluation?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations.
While awaiting clinical evaluation, digestive support supplements may help manage symptom intensity. For GERD-adjacent symptoms, Yuve Probiotic Gummies provide Lactobacillus acidophilus NCFM and Bifidobacterium lactis Bi-07 in a vegan gummy format; preliminary research suggests certain probiotic strains reduce lower esophageal sphincter instability. Digestive Advantage Heartburn Relief (Bacillus coagulans BC30) has been studied for GI symptom reduction. For gallbladder function support, artichoke extract (Cynara scolymus standardized to cynarin) is the best-documented evidence-based supplement for supporting bile flow; a 2016 randomized study in Phytomedicine found meaningful symptom reduction versus placebo. DGL (deglycyrrhizinated licorice) supports esophageal mucosal integrity in GERD; Yuve offers DGL Licorice Chewables. None of these replace diagnostic evaluation.
Best for GERD symptom support: Yuve Probiotic Gummies (Lactobacillus acidophilus NCFM + Bifidobacterium lactis Bi-07)
Best for bile flow support: Artichoke extract (standardized to cynarin, 320–640 mg/day)
Best for mucosal support: DGL licorice (380–400 mg before meals)
FAQ
Can GERD and gallbladder disease occur at the same time?
Yes, they commonly coexist. Population studies find gallstone prevalence elevated in patients with GERD, possibly because both conditions share risk factors including obesity, high-fat diets, and age. When both are present, treatment must address each independently—GERD management with PPIs or lifestyle changes, gallbladder disease through dietary fat restriction and, when indicated, cholecystectomy (surgical removal).
If antacids relieve my pain, does that rule out gallbladder problems?
Not definitively. Antacids reduce gastric acid, which can temporarily ease symptoms that originate from acid irritation of the stomach or esophagus. However, if the primary cause is a gallstone obstructing the bile duct, antacids will not address the underlying obstruction. Relief from antacids increases the probability of an acid-mediated source but does not exclude gallbladder disease, particularly when symptoms recur after fatty meals.
Is gallbladder removal (cholecystectomy) necessary for everyone diagnosed with gallstones?
No. Asymptomatic gallstones (found incidentally on imaging) are generally managed with watchful waiting; about 25% of patients with asymptomatic stones develop symptoms over 10 years. Cholecystectomy is recommended when patients experience recurrent biliary colic, acute cholecystitis, or complications such as pancreatitis. Laparoscopic cholecystectomy is the standard approach with a low complication rate.
What foods worsen both GERD and gallbladder symptoms?
High-fat meals worsen both. For GERD, fatty foods slow gastric emptying and relax the lower esophageal sphincter. For gallbladder disease, high-fat intake triggers cholecystokinin (CCK) release, which contracts the gallbladder and can force stones into the bile duct. Alcohol, caffeine, and carbonated beverages also worsen GERD. Reducing overall dietary fat intake is a shared first-line dietary strategy.
When is upper abdominal pain a medical emergency?
Seek emergency care if upper abdominal pain is severe and persistent (not relieved by position change or antacids), accompanied by fever above 38.5°C (101.3°F), jaundice, inability to keep fluids down, or is associated with chest pain and shortness of breath. Acute cholecystitis, ascending cholangitis, gallstone pancreatitis, and acute coronary syndrome all require urgent evaluation and must not be managed with home remedies.
How do I know if I need an ultrasound vs endoscopy?
An ultrasound is the first test if your dominant symptoms are RUQ pain, fatty meal triggering, and nausea—all pointing toward biliary pathology. An endoscopy (EGD) is prioritized when symptoms are primarily heartburn, regurgitation, hoarseness, and swallowing discomfort—pointing toward the esophagus. Your physician may order both if symptoms are mixed. Both tests are low-risk and the choice depends on your clinical presentation, not symptoms alone.
—
For a deeper look at Yuve’s gut health products, visit the Digestion Collection.
Leave a Reply